Building Interoperable FHIR APIs That Survive Healthcare Vendor Transitions

Here’s a scenario every Health IT leader has lived through: You’ve spent 18 months and $4M integrating your IDN’s clinical and operational systems around your EHR. Every department runs on those integrations. Clinicians depend on them. Then, leadership announces an EHR migration.
And every single one of those integrations has to be rebuilt from scratch. This isn’t a planning failure. It’s an architecture failure. Most health systems build FHIR integrations to vendors, not around an abstraction layer that survives them. When a vendor leaves, everything downstream goes with it.
The good news? There’s a better way to architect FHIR interoperability. One that’s built on open standards, survives vendor transitions, and gets more valuable with every new mandate your organization faces. This guide is for the CTOs, CIOs, and enterprise architects of multi-facility health systems and IDNs who are done rebuilding from zero every time a contract changes.
Why Most FHIR Implementations Don’t Survive Vendor Changes
The Hidden Architecture Problem
Here’s the uncomfortable truth about how most IDNs build FHIR integrations:
They build point-to-point.
Application A calls Epic’s FHIR endpoint. Application B calls Oracle Health. Application C was written for Meditech. Every integration is hardwired to a specific vendor’s implementation of the FHIR standard.
That’s a problem because of one critical fact:
No two EHR vendors implement FHIR the same way.
Epic’s FHIR R4 endpoints behave differently from Oracle Health’s. Custom extensions vary. Authentication scopes differ. Bulk data export behaviors diverge.
So when your IDN migrates from Epic to Oracle Health or acquires a facility running Meditech, your “FHIR-based” integrations don’t port over. They break.
The old integration model was point-to-point: each application required a custom interface to the EHR, maintained by the health system’s IT team. Every new vendor meant another interface, another maintenance burden, and another potential point of failure.
The result?
At most multi-facility health systems, integration rebuild costs during EHR transitions run between $2M and $12M. Timeline overruns are the norm, not the exception. Clinical workflows go dark during cutovers.
And according to Gartner, 83% of data migration projects fail or exceed their budgets and schedules, with healthcare migrations carrying additional patient safety stakes that make failure unacceptable.
Why “FHIR-Ready” Isn’t Enough
Most EHR vendors will tell you their systems are “FHIR-ready.”
They’re not wrong. But they’re not telling the whole story.
“FHIR-ready” means a vendor exposes FHIR R4 endpoints. It does not mean those endpoints are consistent with another vendor’s implementation, fully conform to US Core profiles, or support the full FHIR RESTful API surface your downstream applications need.
Here’s what version fragmentation looks like in the real world:
| EHR Vendor | FHIR Version | Notable Divergence |
| Epic | R4 (primary), DSTU2 (legacy) | Proprietary extensions; SMART on FHIR for app launch |
| Oracle Health (Cerner) | R4 (deprecated DSTU2 Dec 2025) | Millennium-specific resource mapping |
| Meditech | R4 via Greenfield Workspace | Limited write-back support on some resources |
| NextGen | R3 / R4 | Patient access primary use case |
| athenahealth | R4 | Scoped to patient-facing use cases |
The bottom line?
Your integration architecture needs to be vendor-agnostic at its core, and that requires a deliberate abstraction strategy, not a vendor’s “FHIR-ready” checkbox.
The 2026 Regulatory Stack You’re Building Against
Before you design a single endpoint, you need to understand the compliance obligations shaping your architecture decisions right now.
This isn’t background reading. These deadlines have hard teeth.
The Active Mandates
21st Century Cures Act – Information Blocking Rule (Active). Healthcare providers who interfere with the access, exchange, or use of electronic health information face significant penalties. Refusing to support FHIR-based data extraction can constitute information blocking. This is live today.
ONC HTI-1 Final Rule – USCDI v3 via FHIR US Core (January 1, 2026) Certified health IT must support United States Core Data for Interoperability version 3 (USCDI v3) using FHIR US Core profiles. The current US Core Implementation Guide is v9.0.0, based on FHIR R4.0.1. This is the technical baseline for every certified EHR update your vendors must have shipped by now.
What USCDI v3 adds that v1 didn’t cover: social determinants of health data, health insurance information, expanded lab and diagnostic data, and richer medication details. Your integration architecture must accommodate these data elements today.
CMS-0057-F – Interoperability and Prior Authorization Final Rule
This is the big one for IDNs with payer relationships or value-based care contracts.
The phased compliance schedule:
| Requirement | Deadline |
| Prior authorization turnaround rules (operational) | January 1, 2026 |
| First public PA metrics reporting (calendar year 2025 data) | March 31, 2026 |
| Annual API usage metrics to CMS (first report) | March 31, 2026 |
| Patient Access API (with PA data) is live in production | January 1, 2027 |
| Provider Access API is live in production | January 1, 2027 |
| Payer-to-Payer API is live in production | January 1, 2027 |
| Prior Authorization API is live in production | January 1, 2027 |
TEFCA – Trusted Exchange Framework and Common Agreement (Active) TEFCA’s Qualified Health Information Networks (QHINs) are live. Facilitated FHIR exchange was piloted in 2025. Stage 3 FHIR-to-FHIR exchange across QHINs is planned for 2026. Your architecture needs to support QHIN connectivity as a strategic priority, not a future consideration.
A new proposed rule: CMS-0062-P. In 2026, CMS proposed updates to required and recommended FHIR standards and implementation guides to support prior authorization implementation. This signals the regulatory floor will continue rising.
The strategic implication: Every architecture decision you make today needs to be evaluated against a regulatory environment that is accelerating, not stabilizing. Vendor-dependent architectures will require expensive rework every compliance cycle. Vendor-agnostic architectures absorb new mandates at the API layer, without touching downstream applications.
The Vendor-Agnostic FHIR Architecture That Actually Works
The Core Principle: Decouple Your Applications from Your Vendors
This is the architectural shift that changes everything.
Instead of your applications calling vendor endpoints directly, every system in your IDN calls a single FHIR Integration Hub, a vendor-agnostic middle layer that normalizes data, enforces governance, and handles vendor-specific translation internally.
When your EHR changes, only the translation layer needs updating. Your downstream applications don’t know or care what EHR you’re running.
Here’s the reference architecture:
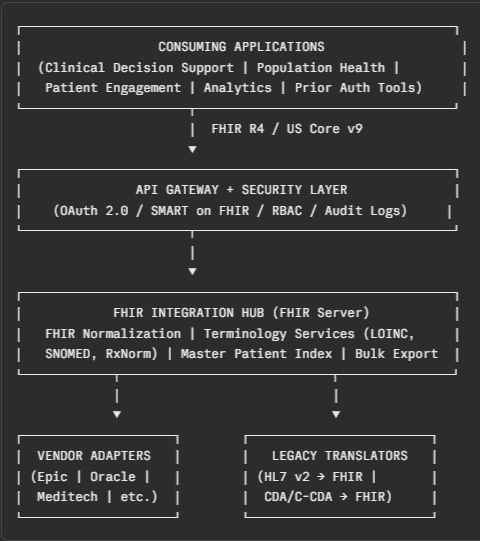
What Each Layer Actually Does
API Gateway + Security Layer
This is your enforcement perimeter.
Every call from every application passes through here. This layer handles:
- OAuth 2.0 + SMART on FHIR for application authentication and authorization
- Role-based access control (RBAC) scoped to patient context, facility, and data element
- Rate limiting and throttling across your integration surface
- Comprehensive audit logging for HIPAA compliance and information blocking defense
Do NOT skip this layer or roll it into your FHIR server. They serve different functions and need to scale independently.
FHIR Integration Hub (Central FHIR Server)
This is the core of your vendor-agnostic architecture.
Think of it as your organization’s FHIR-native operational data store. It maintains a normalized, US Core-compliant representation of patient data across all facilities, independent of which vendor system sourced it. Critical capabilities this layer must provide:
- US Core v9 profile conformance: every resource stored and served must validate against the current US Core profiles
- Terminology services: LOINC, SNOMED CT, RxNorm, and ICD-10 mapping happen here, not in vendor adapters
- Master Patient Index (MPI) integration: patient matching across facilities is your single biggest data quality risk; it must be centralized
- FHIR Bulk Data Export ($export): required for population health, quality reporting, and payer APIs under CMS-0057-F
- FHIR Subscriptions: real-time event-driven notifications as the US Core roadmap progresses toward subscription-based exchange
Vendor Adapters (Isolation Layer)
This is where vendor-specific complexity lives and stays.
Each adapter translates between your FHIR Integration Hub’s normalized data model and a specific EHR vendor’s implementation. Epic quirks, Oracle Health-specific extensions, Meditech’s Greenfield API surface, all of it is encapsulated here.
When you migrate EHRs, you replace one adapter. Everything above it in the architecture is untouched.
This is the architectural decision that makes your FHIR investment survive vendor transitions.
The Patient Identity Problem You Cannot Ignore
One of the toughest barriers in multi-facility IDN architecture is patient identity.
Records from different facilities contain spelling variations, incomplete fields, mismatched dates of birth, and duplicate MRNs. Without a robust MPI strategy, your FHIR integration hub will serve fragmented, unreliable patient data.
The minimum viable approach for an IDN:
- Probabilistic matching with configurable confidence thresholds.
- Centralized Master Patient Index at the integration hub layer (not within individual EHR adapters).
- FHIR Person and Patient resource linkages to maintain cross-facility patient identity.
- Exception workflow for low-confidence matches requiring human review.
Get this right before you go live. A data conversion error in patient records has directly caused clinical harm, one documented incident involved a medication dosage being doubled during a migration. Patient identity is not a data quality problem. It’s a patient safety problem.
HL7-to-FHIR Migration — A Strategy That Doesn’t Break Production
The Hybrid Reality
Here’s something most FHIR guides won’t tell you:
Most large IDNs will run hybrid HL7 v2 + FHIR environments for the next 3–5 years, minimum.
HL7 v2 remains the backbone of many hospital systems, PAS, lab, radiology, and legacy ancillary systems. It’s fast, proven, and deeply embedded. Many of these systems don’t have FHIR-native replacements available today.
The strategic mistake is treating HL7-to-FHIR migration as a big-bang replacement project.
It isn’t. It’s a co-existence strategy with a migration runway.
The Migration Architecture
Your FHIR Integration Hub needs a Legacy Translator component that converts inbound HL7 v2 and CDA/C-CDA documents into FHIR resources in real time.
The translation priorities by volume and risk:
| Legacy Message / Document | FHIR Resource Target | Migration Priority |
| HL7 v2 ADT (patient admit/discharge/transfer) | Patient, Encounter | Immediate — core patient identity |
| HL7 v2 ORU (observation results — labs) | Observation, DiagnosticReport | Immediate — clinical decision support dependency |
| HL7 v2 RDE / RDS (pharmacy orders) | MedicationRequest, MedicationDispense | High — medication reconciliation |
| HL7 v2 ORM / OMG (orders) | ServiceRequest | High — workflow integration |
| CDA / C-CDA documents | DocumentReference, Composition | Medium — care coordination |
| HL7 v2 SIU (scheduling) | Appointment | Lower — operational, not clinical |
The phased migration approach:
- Phase 1: Dual-feed (Months 1–6) Run HL7 v2 feeds to legacy systems, and FHIR feeds to new applications simultaneously. Your legacy translator converts HL7 inbound messages to FHIR resources in the integration hub. New applications consume FHIR-only. Legacy applications continue consuming HL7. Both coexist.
- Phase 2: FHIR Primary (Months 7–18) New integrations are FHIR-only. Legacy systems are queued for retirement or adapter updates. The translator layer remains active but is no longer the primary path for new workflows.
- Phase 3: Legacy Deprecation (Months 19–36) HL7 v2 interfaces are retired system-by-system based on volume and risk priority. Full FHIR-native operations.
Never deprecate an HL7 v2 interface without first validating that the equivalent FHIR resource is passing clinical validation, not just technical conformance testing. Get your clinical informaticists involved. Technical conformance and clinical accuracy are different standards.
API Governance at IDN Scale
Why Governance Fails at Multi-Facility Health Systems
Most IDNs get FHIR technically right and governance wrong.
The symptoms look like this:
- Different facilities use different FHIR profiles for the same resource.
- No versioning strategy, breaking changes are deployed without notice.
- Applications calling endpoints they’re not authorized for.
- No audit trail for who accessed what patient data and when.
- APIs are built for a specific application, then used by others without documentation.
At a single-facility organization, this is manageable. At an IDN with 5, 10, or 20 facilities, it becomes a compliance liability and an operational nightmare.
5 Pillars of FHIR API Governance
1. Profile Governance, US Core as Your Baseline
Establish US Core v9 profiles as the non-negotiable baseline across all FHIR resources in your integration hub. Any extension beyond US Core must go through a formal review process with documented clinical and technical rationale.
Every resource should validate against its US Core profile before being committed to the hub. Automated conformance testing at the pipeline level, not manual review, is the only way to enforce this at the IDN scale.
2. Versioning Strategy
FHIR API versioning is the single most common source of integration breakage during system updates.
Adopt explicit URL-based versioning: /fhir/v1/Patient, /fhir/v2/Patient. Never deploy breaking changes to a live endpoint.
Deprecation policy: a minimum 12-month deprecation window before any versioned endpoint is retired. Notify consuming applications 90 days before any endpoint changes.
3. SMART on FHIR Scoping
Every application that accesses your FHIR Integration Hub must authenticate via SMART on FHIR with explicitly defined OAuth 2.0 scopes.
Scope design principle: minimum necessary access. An application handling prior authorization should not have a scope that allows reading clinical notes. A patient-facing app should not have bulk data export permissions.
Audit your scope assignments quarterly. Over-permissioned applications are your single largest HIPAA exposure in an API-based architecture.
4. API Registry and Documentation
Maintain a centralized API registry, a governed inventory of every FHIR endpoint in your environment, which applications consume it, what scopes they’re authorized for, and what version they depend on.
This isn’t bureaucratic overhead. It’s the document you need when a vendor transition requires you to understand exactly what breaks if a specific endpoint changes.
5. Real-Time Audit Logging
Every FHIR API call must generate an audit log entry that captures: who (user or application), what (resource type and ID), when, from where (IP, facility), and action (read, write, export).
These logs serve two functions: HIPAA compliance and operational intelligence. When a downstream application breaks, your first diagnostic tool is the audit log. When a potential information blocking complaint surfaces, your audit log is your defense.
Key insight for IDN leadership: API governance is not a technical function, it’s an organizational function. The governance framework must have executive sponsorship, defined ownership, and enforcement authority. Technical debt in API governance compounds faster than technical debt in any other system layer because it touches everything.
Future-Proofing — TEFCA, FHIR R6, and What’s Coming
TEFCA: The Architecture Decision You Need to Make Now
TEFCA is live. Qualified Health Information Networks (QHINs) are operational. And Stage 3 FHIR-to-FHIR exchange across QHINs is on the roadmap for 2026.
Here’s what this means for your integration architecture:
Your FHIR Integration Hub is not just an internal enterprise tool. It’s also your front door to the national health data highway.
TEFCA QHIN connectivity requires that your FHIR server support both document-based exchange (for current QHIN operations) and FHIR-based query (for Stage 3 and beyond).
If you’ve built a vendor-agnostic FHIR Integration Hub as described in Chapter 3, TEFCA connectivity is an addition to that architecture, not a rebuild. You’re adding a QHIN interface to a layer that already normalizes and governs your FHIR data.
If you haven’t, TEFCA becomes another expensive point-to-point integration problem.
FHIR R6: What You Need to Know Now
FHIR R6 is expected in late 2026. HL7 International has already released early ballot versions for evaluation.
The critical changes for enterprise architects:
- Most clinical and administrative resources will achieve normative status; this is the stability guarantee that R4 provided for its resources, now extending across a broader surface area. Normative status means no breaking changes without a new major version.
- Reduced future migration complexity, normative R6 resources will have formal backward compatibility guarantees that R5 lacked. This is the version stability that large health systems have been waiting for.
- R5 adoption will likely remain limited; the healthcare industry’s preference for stability means many organizations will skip R5 entirely and plan a direct R4 → R6 transition when the timing is right.
Your action today: Do not build net-new R5 integrations. Build R4 with US Core v9 compliance, monitor the R6 ballot, and design your integration hub to support versioned FHIR endpoints at the gateway layer, so the R4 → R6 transition is a version adapter change, not an architecture rebuild.
The Proposed CMS-0062-P Rule: Plan for Tighter Standards
In 2026, CMS proposed updated requirements for FHIR standards and implementation guides supporting prior authorization.
The direction is clear: the regulatory floor for FHIR implementation will rise again with each rulemaking cycle.
The practical implication for your architecture: compliance automation needs to be built into your CI/CD pipeline, not managed through periodic audits. US Core conformance testing, SMART scope validation, and audit log completeness should be automated quality gates in your FHIR API development process.
The 90-Day Architecture Roadmap
Stop treating FHIR as a compliance checkbox. Start treating it as your strategic integration infrastructure.
Here’s where to focus over the next 90 days:
Days 1–30: Architecture Audit
- Map every active FHIR and HL7 v2 integration in your environment
- Identify which integrations are directly hardwired to vendor endpoints (these are your highest-risk dependencies)
- Validate that your current EHR vendor’s FHIR implementation supports US Core v9 profiles
- Assess your API gateway capabilities. Does it support SMART on FHIR scoping and audit logging at scale?
Days 31–60: Governance Foundation
- Stand up a centralized API registry if one doesn’t exist
- Define and document US Core v9 as your organizational FHIR profile baseline
- Establish OAuth 2.0 / SMART on FHIR scope standards for all API consumers
- Identify your Master Patient Index strategy across facilities
Days 61–90: Architecture Decision
- Decide: Is your current architecture vendor-agnostic at the integration hub layer, or vendor-dependent?
- If vendor-dependent, build the business case for the abstraction layer investment. Use the cost of your last EHR transition rebuild as the baseline ROI calculation.
- If vendor-agnostic: validate TEFCA QHIN connectivity readiness and begin evaluating FHIR R6 ballot implications
The Architecture Principle That Changes Everything
Every FHIR architecture decision comes down to one question:
Does this integration survive the next vendor transition?
If the answer is no, if your architecture is secretly hardwired to a vendor’s proprietary implementation, you’re not building interoperability. You’re buying time.
The health systems that are winning this in 2026 built their FHIR architecture around a vendor-agnostic integration hub before they needed one. When their last EHR transition came, the rebuild cost was a fraction of the industry average. Their downstream applications never went dark.
That’s the outcome a properly governed, standards-based FHIR architecture delivers.
Not just regulatory compliance.
Not just technical checkboxes.
True interoperability that outlasts any single vendor, and gets stronger with every mandate your organization faces.
Quick Reference: FHIR Architecture Decision Checklist
| Architecture Decision | Vendor-Dependent Risk | Vendor-Agnostic Best Practice |
| Application-to-EHR connectivity | Direct vendor endpoint calls | Applications call the central FHIR Integration Hub |
| Patient identity management | Siloed per EHR system | Centralized MPI at the integration hub layer |
| Terminology mapping | Vendor-handled | Centralized terminology services (LOINC, SNOMED, RxNorm) |
| Authentication/authorization | Vendor OAuth implementations | SMART on FHIR at the API gateway layer |
| HL7 v2 translation | Ad-hoc per system | Centralized Legacy Translator in the integration hub |
| US Core conformance | Vendor-certified | Automated conformance validation in the CI/CD pipeline |
| API versioning | None / ad-hoc | Explicit URL versioning with 12-month deprecation windows |
| TEFCA connectivity | Future rebuild required | QHIN interface added to existing integration hub |
| Audit logging | Per-system, siloed | Centralized at the API gateway, every call, every resource |
CapMinds FHIR Interoperability Services: Build Once. Survive Every Vendor Transition.
Your FHIR architecture is only as strong as the team behind it.
CapMinds delivers end-to-end digital healthcare technology services built for multi-facility health systems and IDNs that can’t afford to rebuild from scratch every time a vendor contract changes.
We don’t just implement FHIR. We architect interoperability that lasts.
Our services directly supporting your FHIR strategy include:
- FHIR API Development & Integration: vendor-agnostic integration hub design, US Core v9-compliant resource development, and FHIR R4 endpoint implementation
- HL7-to-FHIR Migration Services: phased migration architecture, legacy translator development, and dual-feed transition management
- EHR Interoperability Solutions: Epic, Oracle Health, Meditech, and athenahealth adapter design and deployment
- Healthcare API Governance Consulting: SMART on FHIR scoping, API registry setup, versioning strategy, and audit logging infrastructure
- CMS-0057-F & ONC HTI-1 Compliance: Patient Access, Provider Access, Payer-to-Payer, and Prior Authorization API delivery
- TEFCA / QHIN Connectivity: FHIR-based nationwide health information exchange readiness
- Enterprise Healthcare Integration Architecture: Master Patient Index strategy, terminology services, and population health infrastructure
- And More. custom digital health solutions tailored to your IDN’s specific integration landscape
Ready to stop rebuilding and start scaling?




