Hybrid Cloud vs Public Cloud: Which One Wins for Healthcare AI Workloads?

Finding AI use cases is rarely difficult for healthcare organizations. Where those workloads should operate is a more difficult topic. Elastic GPU capacity, managed AI services, data platforms, foundation models, and quicker experimentation are all provided via public clouds. Organizations may process data closer to EHRs, imaging systems, medical devices, and clinical workflows that might still be located inside hospital data centers thanks to hybrid cloud. That makes the choice appear straightforward:
- Use public cloud for scale.
- Use hybrid cloud for control.
But that framing is incomplete. A radiology inference service connected to a local PACS has different infrastructure requirements from a claims-denial model running once each night.
A bedside deterioration model has different availability requirements from an internal policy assistant. A research model trained on genomic data creates different data-movement challenges from an AI agent summarizing administrative documents.
The correct decision is not whether the entire organization should use hybrid or public clouds.
The question is: which elements of each healthcare AI workload should operate in the public cloud and which should stay closer to the source data, and how will the business manage both as a single production environment? The workload placement selection has an impact on performance, security, regulatory exposure, cost, resilience, AI governance, and the speed with which a healthcare organization can transition from pilot to production.
What Is Public Cloud for Healthcare AI?
A cloud service provider operates the public cloud, which provides shared infrastructure and platform services. On-demand provisioning is possible for computing, storage, networking, analytics, security, databases, AI models, and machine learning services.
A public-cloud healthcare AI environment may contain:
- Clinical and operational data lakes
- Healthcare data warehouses
- GPU and accelerator instances
- Managed machine learning platforms
- Foundation model services
- Feature stores
- Vector databases
- Model registries
- Batch and real-time inference endpoints
- API gateways
- Identity and access services
- Logging and security monitoring
- Infrastructure-as-code pipelines
- MLOps and model evaluation tools
A public cloud workload is not required to be directly exposed to the public internet. A well-designed healthcare cloud architecture can make use of separated virtual networks, private connectivity, private endpoints, encryption, workload identities, access controls, and centralized monitoring.
HIPAA also does not require electronic protected health information, or ePHI, to be kept within an organization-owned data center. HHS allows covered companies and business associates to use public, private, or hybrid cloud services if they sign an appropriate business associate agreement and comply with all applicable HIPAA requirements. HHS also makes clear that the cloud configuration selected must be considered in the organization’s risk analysis and risk-management process.
What Is Hybrid Cloud for Healthcare AI?
In enterprise healthcare, the term “hybrid cloud” is frequently used in a broad sense. In formal NIST language, hybrid cloud comprises two or more independent cloud infrastructures, such as public and private clouds, that remain separate but are connected by technology facilitating data and application portability.
The phrase is also used more generally in discussions about healthcare architecture to refer to public cloud services that are integrated with:
- Hospital data centers
- Private cloud platforms
- Colocation environments
- On-premises Kubernetes
- Local GPU clusters
- Imaging-center infrastructure
- Medical device environments
- Edge computing platforms
Where the local environment lacks cloud characteristics such as on-demand provisioning, resource pooling, elasticity, and measured services, hybrid IT may be the more technically accurate term.
For this guide, hybrid cloud for healthcare includes an intentionally governed combination of public cloud, private cloud, on-premises, and edge infrastructure used to deliver AI workloads. A functioning hybrid architecture must unify more than network connectivity. It needs consistent approaches for:
- User and workload identity
- Data movement
- Encryption and key management
- Model packaging
- Deployment automation
- Security policy
- Infrastructure provisioning
- Observability
- Incident response
- Cost management
- Backup and recovery
- AI governance
- Audit evidence
Without those controls, the organization does not have one hybrid AI platform. It has multiple disconnected environments with separate operating models and a larger failure surface.
Why Healthcare AI Creates a Different Cloud Decision
Healthcare AI cannot be assessed using the same criteria as a standard online application.
AI workloads rely on enormous datasets, specialized computing, model artifacts, ever-changing software components, and integration with clinical and administrative operations.
Healthcare data has gravity
Healthcare AI data may be distributed across:
- EHR databases
- Clinical data repositories
- PACS
- Vendor-neutral archives
- DICOM imaging studies
- Laboratory systems
- Pharmacy applications
- Medical devices
- Waveform repositories
- Claims platforms
- Contact-center recordings
- Scanned documents
- Genomic repositories
- Remote patient monitoring platforms
- Research databases
A structured patient roster is relatively easy to transfer.
High-resolution medical imaging, digital pathology, genomic data, video, and continuous waveforms can be considerably harder and more expensive to move. The placement decision should evaluate:
- Total data volume
- Daily data growth
- Transfer frequency
- Required retention
- Available bandwidth
- Transfer windows
- Data-transfer costs
- Processing time
- Whether the complete source record is needed
- Whether derived features or selected data elements are sufficient
When data is large, continuously generated, or closely tied to a local application, moving the model closer to the data may be more practical than continually moving the data to the model.
Inference may be more latency-sensitive than training
Model training may tolerate long processing cycles. Production inference may not.
A model predicting appointment demand for the next quarter can run as a scheduled public-cloud workload. An AI application supporting image acquisition, emergency workflows, bedside monitoring, or procedure-room operations may require predictable end-to-end response times.
End-to-end latency includes more than model execution:
- Source-system processing
- Integration-engine processing
- Network travel
- DNS resolution
- Firewall inspection
- API gateway processing
- Retrieval operations
- Model inference
- Output validation
- Destination-system updates
The requirement should therefore be expressed as a measurable service-level objective, such as:
Ninety-five percent of AI results must be available inside the clinical application within two seconds of the triggering event. “Low latency” is not a sufficient architecture requirement.
Healthcare workflows may need to continue during connectivity failure
A public-cloud AI service may remain operational while becoming inaccessible to a hospital because of:
- Carrier failure
- Routing problems
- DNS failure
- Firewall changes
- Private-link failure
- Identity-provider disruption
- Cloud-region connectivity problems
- Local network congestion
For every production AI service, the architecture must define what occurs when the service is unavailable. The workflow may:
- Continue without AI assistance
- Queue requests for later processing
- Use a smaller local model
- Fail over to another connection or region
- Display a degraded-service warning
- Require a manual workflow
- Stop because proceeding would be unsafe
The correct response depends on the clinical and operational consequences of failure. A coding-assistance service and a bedside monitoring model should not have the same downtime design.
AI infrastructure requires lifecycle governance
Healthcare organizations must govern more than servers and storage. They must also govern:
- Training datasets
- Data lineage
- Feature definitions
- Prompt versions
- Retrieval sources
- Model artifacts
- Evaluation datasets
- Model approvals
- Human-review requirements
- Bias and performance assessments
- Drift
- Vendor model changes
- Output monitoring
- Rollback
- Retirement
The NIST AI Risk Management Framework divides AI risk management into four functions: governance, mapping, measurement, and management. It is optional, but it provides a valuable framework for administering healthcare AI in the public cloud, on-premises, and edge contexts.
Hybrid Cloud vs Public Cloud for Healthcare AI
| Decision area | Public cloud | Hybrid cloud or hybrid IT |
| Speed to pilot | Usually faster because managed services and compute can be provisioned rapidly | May require local hardware, networking, security, and platform preparation |
| Elastic model training | Strong fit for temporary or variable GPU demand | Can combine local capacity with cloud bursting, but local capacity remains finite |
| Local inference | Depends on cloud connectivity and end-to-end network performance | Can place inference closer to EHRs, PACS, devices, and clinical applications |
| Data movement | May require large or continuous transfers | Can retain high-volume data locally and transfer only approved outputs or features |
| Managed AI services | Broad foundation-model, analytics, data, and MLOps ecosystems | Service availability may be narrower or platform-dependent |
| Operational complexity | Lower when managed services are used effectively | Higher because multiple infrastructure, network, identity, and deployment environments must be operated |
| WAN interruption | Requires resilient connectivity, failover, queuing, or downtime workflows | Can support local continuity, but only when the specific product and application support it |
| Security boundary | Primarily concentrated in the cloud landing zone and connected systems | Expanded across cloud, local sites, edge locations, connectivity, and management planes |
| Cost structure | Consumption, storage, data transfer, models, logging, connectivity, and support | Cloud costs plus hardware, facilities, lifecycle management, staffing, redundancy, and support |
| Legacy integration | Requires reliable connectivity to local systems | Can place integration and inference closer to legacy applications |
| Portability | Managed services may create provider dependencies | Containers improve consistency, but data, identity, observability, and managed-service dependencies remain |
| Best fit | Elastic, cloud-native, managed-service-oriented workloads | Workloads with local data, latency, continuity, device, or integration constraints |
Which Healthcare AI Workloads Commonly Fit Public Cloud?
Public cloud is generally the better starting point when a workload benefits from elasticity, centralized processing, rapid experimentation, or managed AI services.
Large or irregular model training
Training workloads often need high computing capacity for a limited period.
Public cloud can reduce the need to purchase hardware for peak demand when teams need to:
- Test several model architectures
- Run temporary distributed training
- Fine-tune foundation models
- Process large research datasets
- Compare different GPU types
- Expand capacity for a specific development cycle
This financial advantage depends on disciplined resource controls. Unscheduled notebooks, idle GPU clusters, forgotten endpoints, and excessive logging can quickly reduce the economic benefit.
Generative AI development
Public cloud commonly provides faster access to:
- Foundation models
- Managed inference endpoints
- Vector search
- Evaluation tools
- Guardrail services
- Agent frameworks
- Development environments
- Model monitoring
- API management
Potential healthcare use cases include:
- Clinical document summarization
- Coding assistance
- Denial analysis
- Contact-center support
- Prior authorization document preparation
- Internal knowledge search
- Policy assistance
- Patient communication drafting
Before PHI enters a service, the organization must verify the BAA, service eligibility, data retention, logging, regional availability, model-training terms, support access, and configuration responsibilities.
A BAA with a cloud provider does not mean every product, model, preview feature, or third-party service available through that provider can automatically process PHI.
Population health and enterprise analytics
Centralized cloud platforms can support data aggregation across hospitals, clinics, service lines, and source systems.
Common workloads include:
- Risk stratification
- Care-gap analysis
- Readmission modeling
- Length-of-stay analysis
- Denial prediction
- Staffing forecasts
- Supply chain optimization
- Quality measurement
- Network-level operational analytics
These workloads normally prioritize scalable processing and cross-enterprise visibility over subsecond local response.
Choose the Right Cloud Model for Every AI Workload
Assess data location, latency, GPU demand, security, integration, and operating cost before committing to public or hybrid cloud infrastructure.
Which Workloads Commonly Fit Hybrid Architecture?
Hybrid architecture becomes more compelling when AI must remain close to local data, clinical systems, devices, or time-sensitive workflows.
Imaging inference
Medical imaging workflows may involve large files and direct integration with:
- PACS
- Vendor-neutral archives
- Imaging modalities
- Worklists
- Reporting systems
- DICOM routers
A hybrid design may process images locally while using public cloud for centralized model development, evaluation, governance, and long-term analytics.
However, local inference should not be assumed automatically. Public-cloud inference can still be appropriate when measured bandwidth, latency, workflow continuity, security, and image-routing requirements are satisfied.
Bedside and device-connected inference
Local or edge processing may be appropriate for:
- Real-time waveforms
- Medical device data
- Procedure-room video
- Smart-room applications
- Local speech processing
- Remote sites with unreliable connectivity
- High-frequency physiologic monitoring
These workloads may require predictable response times or continued operation when cloud connectivity is degraded. The organization must still determine whether identity, licensing, logging, model serving, and management functions continue during an outage.
Legacy clinical-system integration
Many health systems still operate EHR modules, departmental applications, databases, imaging systems, and interface engines within their data centers.
Local integration components can reduce network hops between:
- The source system
- The AI service
- The integration layer
- The clinical application
- The destination work queue
This may improve reliability when the legacy system cannot support modern cloud-native integration patterns.
Controlled local data processing
Organizational policy, research agreements, intellectual-property restrictions, contractual terms, or risk analysis may justify local processing.
The organization might keep source data local while sending only approved:
- De-identified information
- Aggregated results
- Derived features
- Model updates
- Performance telemetry
- Non-sensitive metadata
Prompts, outputs, logs, embeddings, and derived data should not automatically be assumed to be outside PHI or privacy requirements.
Healthcare AI Workload-Placement Matrix
| Workload | Common starting architecture | Key placement considerations |
| Foundation-model experimentation | Public cloud | Managed models, speed, elasticity, data handling |
| Temporary large-scale training | Public cloud | GPU demand, training duration, data-transfer cost |
| Population health analytics | Public cloud | Centralized data, batch processing, enterprise scale |
| Administrative AI agents | Public cloud | Managed models, variable demand, workflow integrations |
| Ambient documentation | Public cloud or hybrid | Audio handling, EHR integration, latency, downtime |
| Radiology model training | Public cloud or hybrid | Imaging volume, research controls, transfer economics |
| Real-time radiology inference | Hybrid or public cloud | Measured latency, PACS integration, bandwidth, continuity |
| Bedside or device inference | Hybrid or edge | Local response, device integration, outage behavior |
| Genomics and research | Public cloud or hybrid | Dataset size, collaboration, compute demand, agreements |
| Federated or distributed learning | Hybrid | Node security, aggregation, privacy, poisoning resistance |
| Claims and revenue cycle models | Public cloud | Batch processing, centralized data, demand variability |
| Operational command-center AI | Public cloud or hybrid | Source-system integration, criticality, connectivity |
These are starting patterns, not universal rules.
Final placement depends on measured requirements, the location of authoritative data, the regulatory status of the AI function, network resilience, operational capabilities, and the consequence of failure.
Architecture Pattern: Central Governance, Distributed Inference
For many large healthcare organizations, the strongest model is:
Develop, evaluate, approve, and govern centrally, then deploy inference where the workflow requires it.
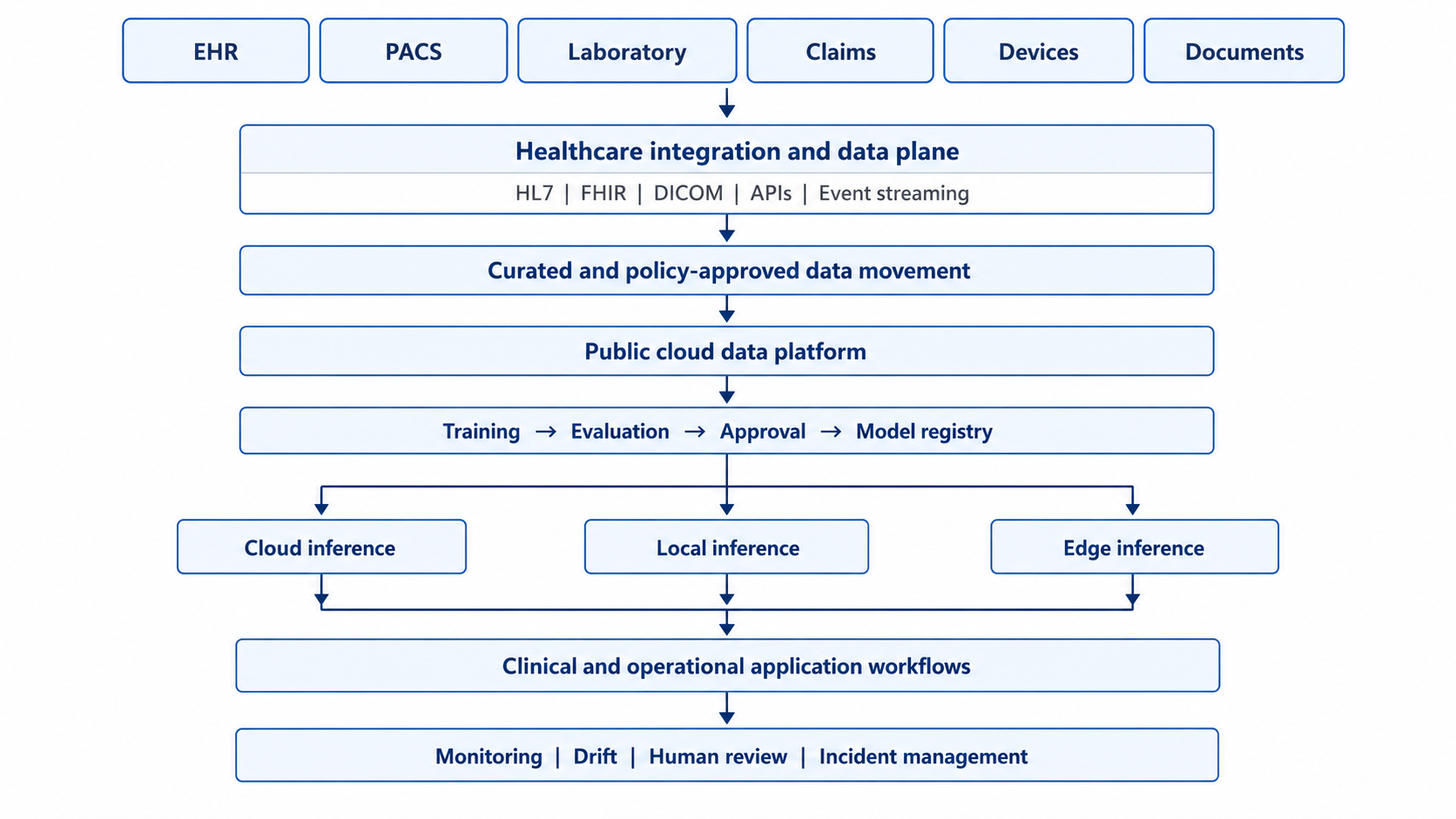
Cross-cutting controls must operate across the architecture:
- User and workload identity
- Encryption and key management
- Data lineage
- Consent and authorization
- Model approval
- Policy enforcement
- Security monitoring
- Cost management
- Compliance evidence
- Human oversight
This architecture separates two decisions:
- Where should a model be developed, evaluated, and governed?
- Where should inference run?
The answers do not have to be the same. Microsoft documents Azure Arc as a way to provide unified management and governance across public-cloud, on-premises, and multicloud machine learning environments.
Google Distributed Cloud provides Vertex AI capabilities in an air-gapped environment. AWS Outposts extends selected AWS infrastructure and services to customer premises.
These products do not have identical operating models.
AWS Outposts requires a service-link connection to its home AWS Region for management and regional communication. Google Distributed Cloud air-gapped is designed for isolated environments. Microsoft Foundry Local introduced disconnected deployment support in June 2026, but the product remains in preview as of July 2026.
“Runs locally” and “continues operating independently of the cloud control plane” are not equivalent requirements.
Is Hybrid Cloud More HIPAA Compliant?
No. Hybrid cloud is not automatically more compliant because infrastructure is installed inside a hospital. Public cloud is not automatically compliant because a cloud provider offers a BAA.
HHS allows regulated entities to use public, private, and hybrid cloud services, but the covered entity or business associate remains responsible for understanding the environment, conducting a risk analysis, and meeting applicable HIPAA requirements. A cloud service provider that maintains encrypted ePHI can still be a business associate even when it cannot decrypt the information.
A healthcare AI architecture should address:
- Security risk analysis
- Appropriate BAAs
- Verification of covered services
- User and workload identity
- Least-privilege access
- Network segmentation
- Encryption
- Key management
- Secrets management
- Data classification
- Data minimization
- Audit logging
- Vulnerability management
- Backup and recovery
- Incident response
- Downtime procedures
- Vendor risk
- Secure deletion
- Model and artifact integrity
NIST zero trust guidance states that trust should not be granted solely because a user, device, or service is located inside an enterprise network.
That principle is especially important in hybrid healthcare environments, where on-premises location should not substitute for continuous authentication, authorization, and policy enforcement.
HIPAA is not the full regulatory perimeter
The legal and contractual scope may extend beyond HIPAA.
Depending on the data and intended use, organizations may need to evaluate:
- 42 CFR Part 2
- FDA medical device requirements
- FTC health privacy requirements
- State consumer health-data laws
- Human-subject research requirements
- Data-use agreements
- Payer and provider contracts
- Intellectual-property restrictions
The updated 42 CFR Part 2 final rule applies to records maintained in connection with applicable substance use disorder programs, with compliance required beginning February 2026. Certain protections remain stricter than general HIPAA treatment, including restrictions on using SUD treatment records to investigate or prosecute patients without consent or an appropriate court order.
The FTC Health Breach Notification Rule can apply to certain health applications, connected devices, and similar products that are not covered by HIPAA.
Workload classification must occur before cloud-service selection or data movement.
When a Healthcare AI Workload May Be a Medical Device
Not every healthcare AI application is a medical device.
However, an AI function used for diagnosis, monitoring, prediction, treatment, or other medical purposes may require an FDA regulatory assessment.
Cloud architecture then becomes part of product lifecycle control.
Changes to the following may affect validated or authorized behavior:
- Model version
- Training data
- Decision threshold
- Input features
- Preprocessing
- Inference runtime
- Hardware
- Deployment environment
- Output presentation
- Integration logic
FDA maintains a list of AI-enabled medical devices authorized for marketing in the United States.
In August 2025, FDA issued final guidance on predetermined change control plans for AI-enabled devices, including planned modifications, methods for developing and validating changes, and assessments of their effects. The MLOps process should therefore account for:
- Regulatory status
- Validated model versions
- Approved changes
- Site-specific validation
- Deployment approval
- Change control
- Post-deployment monitoring
- Rollback
- Auditability
A cloud platform should not automatically replace or update a regulated model simply because a newer version is available.
Preview Services and PHI Require Extra Scrutiny
Hybrid AI platforms are changing rapidly in 2026.
Some local inference, agentic retrieval, and distributed AI capabilities remain preview or pre-general-availability products.
Preview services may have:
- Limited support
- Changing APIs
- Incomplete service-level commitments
- Product limitations
- Different contractual terms
- Restricted regional availability
- Uncertain PHI eligibility
Google instructs HIPAA-regulated customers not to use pre-GA offerings with PHI unless the specific offering’s notice or terms expressly allow it. Google also places responsibility on customers to use covered services and configure them appropriately.
Microsoft identifies Foundry Local and its Agentic Retrieval capability as preview products as of July 2026.
Before using any new AI model, local inference extension, vector service, agent framework, or distributed-cloud feature with PHI, verify:
- BAA coverage
- Product eligibility
- General-availability status
- Support terms
- Data retention
- Logging behavior
- Regional availability
- Model-training terms
- Service-level commitments
- Security limitations
- Upgrade and retirement policies
Cost Question: Public Cloud vs Hybrid
A valid cost comparison cannot compare a public-cloud invoice only with the purchase price of local servers.
Public-cloud costs can include:
- GPU and accelerator usage
- CPU and memory
- Storage
- Data transfer
- Foundation-model API use
- Vector databases
- Real-time endpoints
- Logging
- Security tools
- Private connectivity
- Backup
- Reserved capacity
- Software licensing
- Support
- Platform engineering
Hybrid costs can include:
- GPU servers
- Storage
- High-performance networking
- Hardware support
- Power and cooling
- Data center space
- Depreciation
- Replacement cycles
- Platform licenses
- Cloud connectivity
- Public-cloud consumption
- Patching
- Firmware management
- Backup
- Redundancy
- Security tooling
- On-call operations
- Platform staffing
Public cloud is often financially attractive for experimental, bursty, or uncertain demand.
Dedicated local capacity may become economical for stable, highly utilized workloads, but only when the organization can maintain high utilization and operate the platform reliably. Measure:
- Cost per completed training run
- Cost per accepted model
- Cost per 1,000 inferences
- Cost per processed study
- Cost per summarized encounter
- Cost per generated token
- Cost per concurrent user
- GPU utilization
- Idle capacity
- Support effort
- Recovery cost
The environment with the lowest compute rate may still have the highest total operating cost.
Production Acceptance Criteria for Healthcare AI Infrastructure
Before finalizing workload placement, define measurable gates.
| Area | Example acceptance criterion |
| Latency | P95 and P99 end-to-end response time |
| Availability | Monthly service availability target |
| Connectivity | Maximum tolerated WAN interruption |
| Recovery | Documented RTO and RPO |
| Scale | Peak and sustained inference volume |
| Data movement | Daily transfer volume and transfer window |
| Compute | Minimum sustained GPU utilization |
| Reliability | Maximum failed-request rate |
| Integration | Maximum failed interface or API transaction rate |
| Model quality | Approved performance threshold by use case |
| Human oversight | Percentage of outputs requiring review |
| Drift | Trigger threshold for investigation or rollback |
| Rollback | Maximum time to restore the prior model |
| Cost | Maximum cost per inference, study, or encounter |
| Security | Required identity, encryption, and logging controls |
| Continuity | Tested degraded-mode and downtime workflow |
These criteria make cloud placement defensible and testable.
Healthcare AI Cloud Modernization Approach
Phase 1: Inventory the AI portfolio
Document each use case’s:
- Business owner
- Intended purpose
- Data sources
- PHI exposure
- Model type
- Integration requirements
- Latency
- Availability
- Risk level
- Expected demand
- Regulatory status
- Operating owner
Phase 2: Build the cloud foundation
Establish:
- Cloud landing zones
- Account structures
- Identity federation
- Network segmentation
- Private connectivity
- Encryption and key management
- Centralized logging
- Infrastructure as code
- Policy as code
- Backup and recovery
- Cost allocation
Phase 3: Build the healthcare data plane
Create repeatable patterns for:
- HL7
- FHIR
- DICOM
- X12
- Documents
- Device data
- Patient identity
- Provider identity
- Terminology normalization
- Data quality
- Lineage
- Consent
- De-identification
- Retention
Phase 4: Standardize MLOps and GenAIOps
Govern:
- Source code
- Training data
- Feature versions
- Prompts
- Retrieval sources
- Models
- Evaluation results
- Deployment targets
- Monitoring
- Drift
- Incidents
- Rollback
Phase 5: Test two architecture patterns
Pilot:
- One public-cloud-oriented workload
- One workload with local or edge inference requirements
This validates whether the operating model works across both environments.
Phase 6: Apply production gates
Require:
- Security review
- Privacy review
- Regulatory assessment
- Architecture approval
- Workflow validation
- Performance testing
- Failure testing
- Recovery testing
- Monitoring
- Cost approval
- Support ownership
- Rollback planning
Phase 7: Optimize using production evidence
Track:
- Adoption
- Latency
- Model quality
- Override rates
- Failed requests
- GPU utilization
- Cloud spending
- Cost per inference
- Drift
- Incidents
- Support effort
- Workflow impact
Infrastructure decisions should change when production evidence changes.
Common Healthcare AI Cloud Mistakes
Choosing hybrid cloud only because data contains PHI
Properly governed public cloud services can process ePHI. Data classification should determine controls, not automatically determine location.
Assuming local infrastructure is safer
On-premises systems may have weak segmentation, incomplete logging, inconsistent patching, shared accounts, or inadequate redundancy.
Buying GPUs before measuring demand
Local AI hardware can become an underutilized asset when model choices, priorities, or development schedules change.
Treating Kubernetes as the hybrid strategy
Kubernetes does not solve data architecture, identity, governance, observability, model lifecycle, or disaster recovery.
Ignoring control-plane dependencies
A local inference service may still depend on cloud identity, DNS, licensing, model registries, logging, or management services.
Assuming federated learning guarantees privacy
Federated learning can keep source data local, but model updates, participating nodes, aggregation, metadata, and poisoning risks still require controls.
Using one architecture for every AI workload
Administrative assistants, imaging models, device applications, and regulated clinical AI require different controls and placement decisions.
Final Verdict: Which One Wins?
Public cloud wins when healthcare AI needs:
- Elastic compute
- Rapid experimentation
- Managed AI services
- Centralized analytics
- Temporary GPU capacity
- Simpler infrastructure operations
Hybrid cloud or hybrid IT wins when workloads have measurable requirements involving:
- Local data gravity
- Predictable latency
- Medical device integration
- Legacy system proximity
- Workflow continuity
- Disconnected operation
- Contractual or research restrictions
- Stable high-utilization local compute
For many enterprise health systems, the best portfolio architecture will be hybrid. But that does not mean every workload belongs on-premises.
The strongest strategy is:
- Use public cloud as the preferred environment for development, training, centralized governance, and managed AI services.
- Deploy local or edge processing only when measurable requirements justify it.
- Govern all environments through consistent identity, security, MLOps, observability, and incident management.
- Validate failure behavior before production.
- Measure performance and cost at the workload level.
The winner is not the environment that hosts the most AI workloads.
It is the architecture that places each workload where it can operate safely, reliably, economically, and close enough to the healthcare workflow to create measurable value.
CapMinds Healthcare AI Cloud Architecture Services
Turn your healthcare AI cloud strategy into a secure, production-ready operating environment with CapMinds. We help health systems, healthcare organizations, and digital health companies assess workloads, modernize infrastructure, integrate clinical data, and deploy AI across public cloud, private cloud, on-premises, and edge environments.
Our end-to-end services include:
- Healthcare AI workload placement and cloud readiness assessments
- Public, hybrid, private, and multicloud architecture
- Healthcare cloud migration and infrastructure modernization
- Secure cloud landing zones, identity, zero trust, and network design
- AI/ML platform engineering, MLOps, model governance, and observability
- EHR, HL7, FHIR, DICOM, API, laboratory, claims, and device integration
- Healthcare data platforms, data pipelines, migration, and modernization
- HIPAA security risk assessments, cybersecurity, compliance support, and disaster recovery
- GPU infrastructure planning, AI FinOps, performance optimization, and cost control
- Managed cloud operations, NOC monitoring, application support, and more
From architecture assessment through implementation and ongoing operations, CapMinds provides one accountable service partner across cloud, data, AI, interoperability, security, and healthcare workflows.
We align each workload with the right deployment model while reducing integration risk, operational fragmentation, and avoidable infrastructure spending, without forcing every workload into the same cloud environment.
Schedule a Healthcare AI Cloud Strategy Call to build a practical roadmap for your next AI workload.