Why Lift-And-Shift Healthcare Cloud Strategies Often Backfire

Lift-and-shift, also known as rehosting, is a cloud migration approach in which an organization moves an existing application, database, operating system, and server configuration from an on-premises environment to cloud infrastructure with little or no application modification. It is commonly selected because it can reduce migration complexity, shorten the initial timeline, and help organizations exit aging data centers without immediately redesigning legacy applications.
For healthcare organizations, this may involve moving an EHR application, interface engine, billing platform, clinical database, imaging gateway, or reporting system onto cloud-hosted virtual machines while retaining its existing architecture and integrations.
However, lift-and-shift is only one migration option. Other approaches include replatforming, where selected components are moved to managed cloud services; refactoring or rearchitecting, where the application is redesigned for cloud capabilities; replacing, where the legacy system is exchanged for another platform; and retaining or retiring workloads that should not be migrated.
The problem begins when healthcare organizations use lift-and-shift for every workload without evaluating security, interoperability, latency, resilience, compliance, and long-term operating costs.
The Core Problem: Cloud Infrastructure Does Not Fix Application Architecture
A legacy EHR module, PACS workflow, interface engine, billing platform, or analytics application may depend on static IP addresses, local Active Directory groups, shared file systems, server affinity, hard-coded URLs, database-linked servers, scheduled jobs, or low-latency access to systems that remain on-site.
Rehosting preserves these dependencies. The organization gains cloud hosting while still managing operating systems, patching, middleware, certificates, database tuning, backups, and failover.
6 Ways Lift-and-Shift Backfires in Healthcare
1. Hidden Dependencies Become Production Outages
Healthcare applications exchange ADT, ORM, ORU, SIU, DFT, X12, C-CDA, FHIR, DICOM, and proprietary traffic with EHRs, labs, pharmacies, PACS, clearinghouses, HIEs, identity systems, and devices.
A server inventory does not expose these transaction-level dependencies. Assessment must identify:
- Data flows and interface directions
- Ports, protocols, DNS records, and firewall rules
- Certificates and service accounts
- Peak transaction volumes and batch windows
- Upstream and downstream system owners
- Retry, acknowledgement, and message-replay behavior
Google’s migration guidance treats workload inventory, dependency cataloging, proof-of-concept testing, total cost of ownership analysis, and migration-plan validation as essential assessment activities.
When this work is skipped, failures appear after cutover as delayed results, duplicate messages, inaccessible documents, broken charge feeds, or intermittent authentication errors.
2. Clinical Latency Is Treated Like Generic Application Latency
A system can pass infrastructure testing and still fail clinically. Several additional seconds can make chart opening, image retrieval, medication reconciliation, or order entry unacceptable.
The correct test is not:
Can the server respond? The correct test is:
Can the complete clinical transaction meet its service-level objective under normal and peak load?
Measure latency across the user device, site network, identity provider, application tier, integration layer, database, storage, and external endpoints.
For example, a diagnostic image workflow may cross:
Clinical workstation → WAN → cloud application → identity service → PACS gateway → image repository → viewer
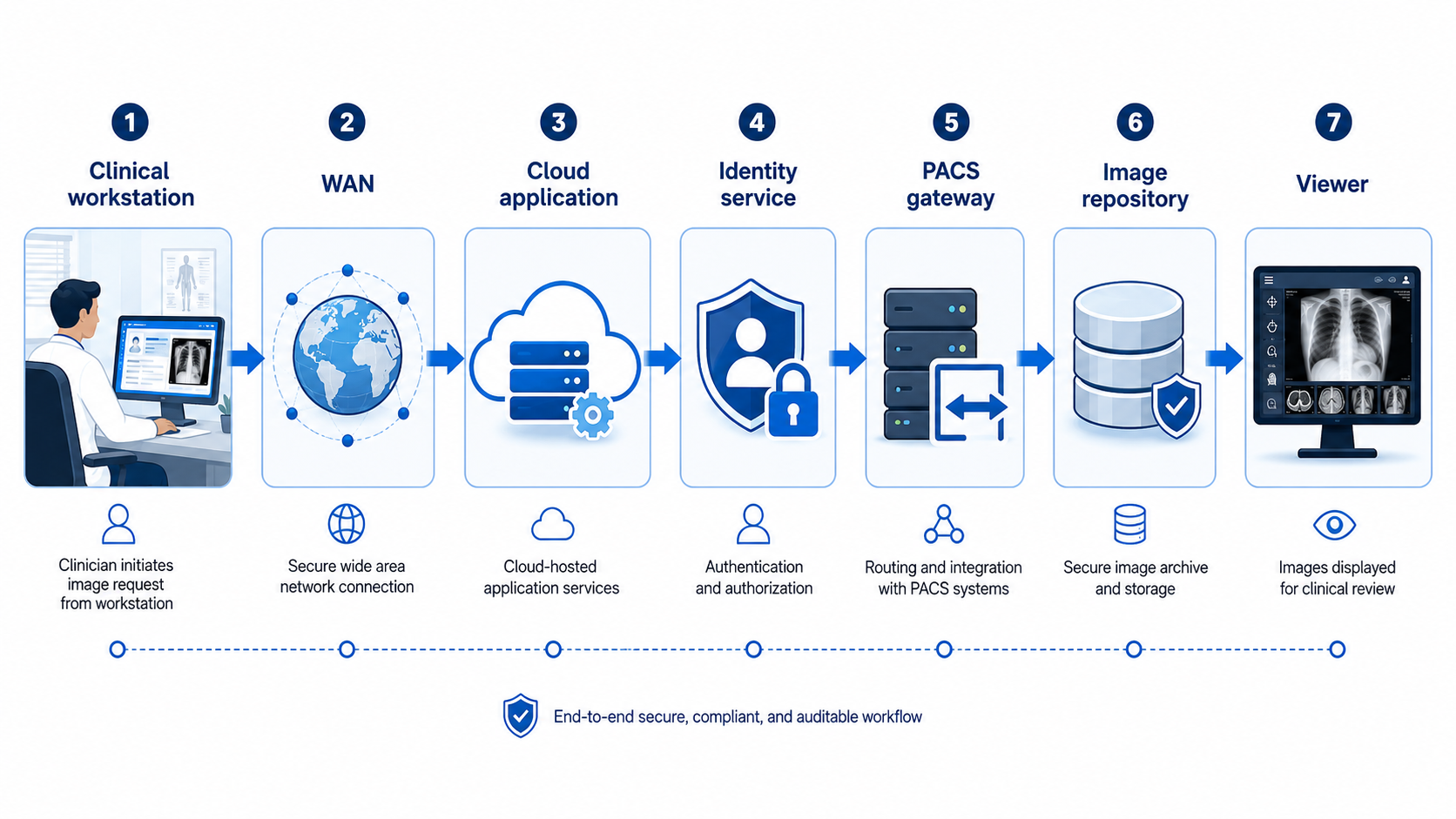
Testing only the cloud virtual machine misses most of that transaction.
Multi-site healthcare organizations also need resilient network connectivity because cloud availability cannot compensate for a failed clinic, hospital, or ambulatory-site network path.
3. On-Premises Trust Models Are Copied Into the Cloud
Replicating a flat internal network can create oversized subnets, permissive security rules, shared administrator accounts, long-lived credentials, and excessive east-west access.
NIST zero-trust guidance rejects implicit trust based on network location and emphasizes policy-based, per-resource access. Cloud providers also use shared-responsibility models: the provider secures the underlying infrastructure, while the customer remains responsible for identity, application configuration, customer data, and many network controls.
Moving electronic protected health information to cloud infrastructure does not remove HIPAA obligations.
HHS states that regulated organizations must:
- Execute an appropriate business associate agreement with a cloud service provider that creates, receives, maintains, or transmits ePHI
- Conduct their own security risk analysis
- Establish risk-management policies appropriate to the cloud configuration
- Ensure contractual service terms do not prevent appropriate access to ePHI
A cloud provider’s HIPAA-eligible services or certifications do not automatically make the deployed workload compliant.
4. The On-Premises Cost Model Is Duplicated
On-premises servers are often sized for infrequent peaks and left running continuously. A one-to-one virtual machine copy carries that overprovisioning into a metered environment.
Costs also include:
- Storage tiers and provisioned IOPS
- Snapshots and backup retention
- Inter-zone or outbound data transfer
- Operating system and database licensing
- Security and observability platforms
- Development and testing environments
- Standby replicas and idle recovery capacity
Cost control starts with utilization data, not source-server specifications.
AWS recommends assessing resource-utilization patterns and peak loads to select appropriate instance types and sizes. Google recommends aligning resources with each workload’s availability, scalability, security, and performance requirements.
A server configured with 32 virtual CPUs on-premises may not need an equivalent cloud instance. Conversely, a database with modest average CPU utilization may still require high storage throughput during claims processing, interface bursts, report generation, or overnight batch activity.
5. Rehosting Is Mistaken for High Availability
A virtual machine in one availability zone remains a single-location workload.
Unless the application, database, file share, integration layer, and network path are designed for redundancy and tested for failover, the migration only relocates the single point of failure.
AWS identifies single-zone production deployment as an architectural anti-pattern. NIST contingency-planning guidance requires organizations to determine recovery priorities and establish viable recovery procedures.
Define the following before cutover:
- Recovery time objective
- Recovery point objective
- Database consistency requirements
- Interface queue and replay procedures
- Clinical downtime workflows
- Failover decision authority
- Failback and reconciliation procedures
Backups are not equivalent to disaster recovery.
A backup is useful only when the organization can restore it within the required recovery window and confirm that clinical, financial, and interface data remain consistent.
6. Technical Debt Becomes Harder to Remove
Unsupported operating systems, tightly coupled modules, undocumented jobs, proprietary integrations, and obsolete databases do not become modern because they run on cloud compute.
Rehosting can delay remediation because the migration is reported as complete.
AWS modernization guidance notes that rehosting alone does not produce faster feature delivery, improved service levels, or fewer unplanned outages. Modernization requires functional, technical, financial, and organizational assessment.
A Safer Healthcare Cloud Migration Pattern
Refactoring every workload before moving can create excessive scope and clinical risk. Use selective modernization based on criticality, dependency complexity, and operational value.
Step 1: Map Clinical and Technical Dependencies
Inventory applications, databases, interfaces, devices, vendors, certificates, service accounts, batch jobs, data classifications, and owners.
Map each critical workflow from the initial user action to downstream confirmation.
Step 2: Define Requirements Before Selecting Cloud Services
Document:
- Availability targets
- Peak concurrency and transaction volumes
- Acceptable workflow latency
- RTO and RPO requirements
- Data retention and auditability
- Encryption and key-management requirements
- Downtime procedures
- Support and escalation paths
These requirements determine the target architecture. The source server configuration does not.
Step 3: Establish the Cloud Foundation
Create governed accounts, segmented networks, private connectivity, centralized identity, privileged access, key management, logging, monitoring, backup policy, configuration baselines, tagging, and budget controls before production arrives.
A healthcare cloud landing zone should support the following control path:
Users and clinical sites → identity and access controls → protected network ingress → application services → interoperability layer → healthcare data services
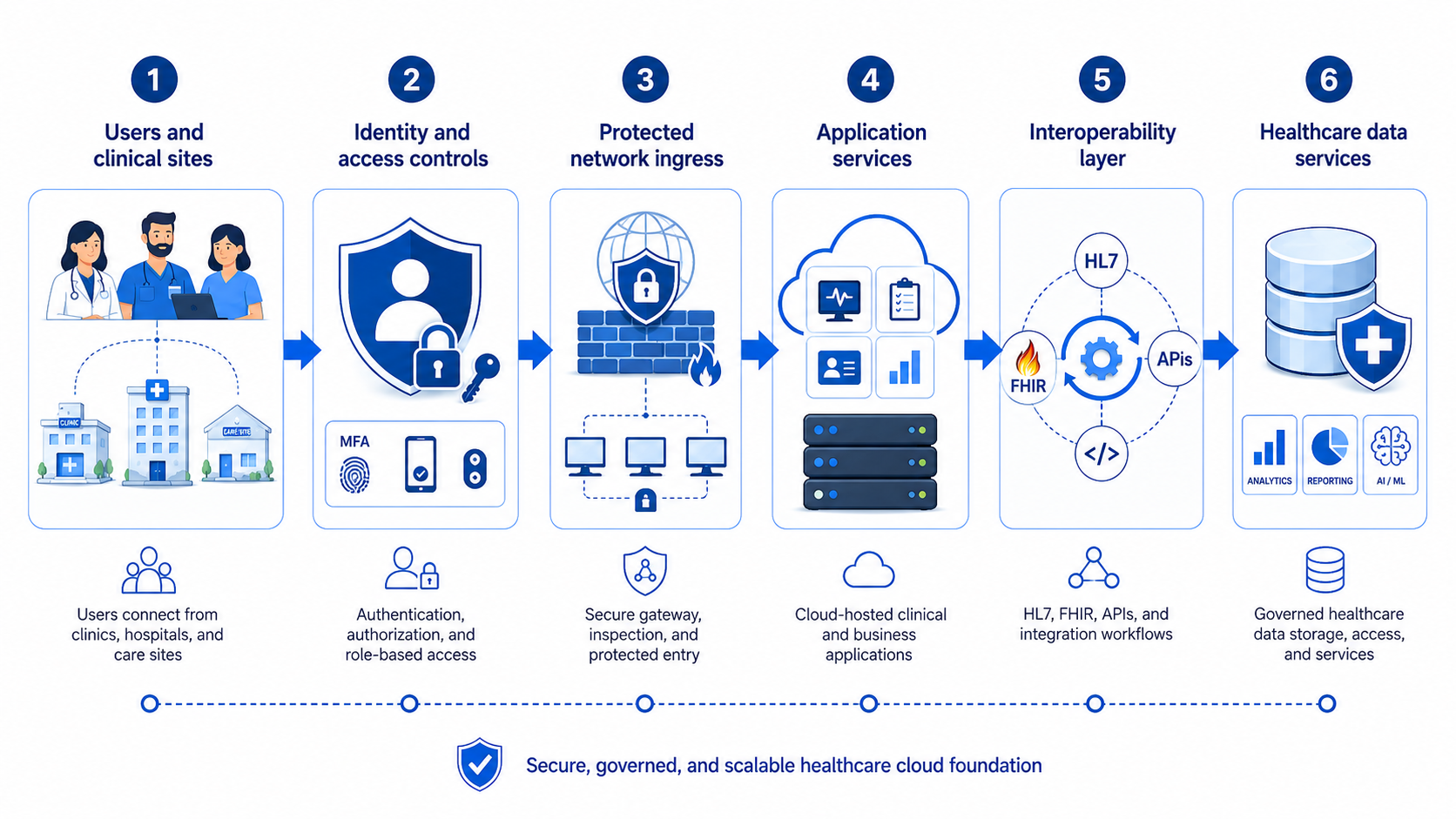
Security monitoring, audit logging, backup, disaster recovery, configuration management, and cost governance should apply across every layer.
Step 4: Choose a Strategy Per Workload
Use rehost for stable, low-dependency workloads needing rapid relocation.
Use replatform when managed databases, storage, backup, messaging, or container services can reduce operational risk without major application changes.
Use refactor when components prevent required resilience, security, scalability, or interoperability.
Use retain when a workload requires local device proximity, cannot tolerate network latency, or lacks a safe migration path.
Use retire when the application no longer provides sufficient clinical, operational, or financial value.
Step 5: Pilot Complete Workflows
Test registration, ordering, results, image retrieval, medications, claims, document access, identity, interface replay, restoration, peak load, and site-connectivity failure.
Testing only the migrated server misses the clinical transaction.
Step 6: Cut Over With Reconciliation and Rollback
Use migration waves, freeze windows, replication checkpoints, message-queue controls, database reconciliation, interface count validation, user acceptance criteria, command-center ownership, and a rehearsed rollback plan.
A rollback document that has never been tested is not an operational rollback capability.
Step 7: Stabilize, Measure, and Optimize
Compare latency, errors, utilization, availability, security events, and spend with baselines.
After stabilization:
- Rightsize compute and storage
- Remove temporary migration infrastructure
- Automate patching and configuration checks
- Improve application and interface observability
- Validate backup res
Infrastructure-as-code is valuable, but a generic template cannot encode an organization’s clinical workflows, vendor constraints, BAA boundaries, recovery priorities, interface behavior, or patient-safety tolerances. The buyer needs a validated migration blueprint and execution plan, not isolated code that appears complete outside its production context.
Build a Healthcare Cloud Strategy That Improves the Workload
CapMinds helps healthcare organizations assess application portfolios, map clinical dependencies, design secure landing zones, select migration strategies, modernize high-risk components, validate interoperability, and operate cloud environments after cutover.
Our healthcare cloud, security, managed IT, and consulting services address:
- Healthcare cloud readiness and workload assessment
- Cloud architecture and landing-zone design
- Application migration and modernization
- EHR, HL7, FHIR, DICOM, and API integration
- HIPAA security and risk controls
- Cloud monitoring, backup, and disaster recovery
- Managed infrastructure and post-migration optimization
- And more
Do not move technical debt and call it transformation.
Talk to CapMinds for a healthcare cloud readiness assessment and a phased migration plan built around your clinical, compliance, interoperability, reliability, and financial requirements.




