MDR, XDR, and SIEM Architecture Patterns For Healthcare SOC Modernization

Healthcare SOC modernization is not simply a matter of replacing a legacy SIEM or adding an XDR platform. The real challenge is correlating identity events, endpoint alerts, cloud activity, EHR audit logs, interface-engine events, medical-device traffic, and network telemetry without introducing new risks to patient care.
A mature healthcare SOC must answer four questions:
- What happened?
- Which user, device, application, or clinical service is affected?
- Can the threat be contained without disrupting care delivery?
- What evidence must be preserved for investigation and compliance?
HIPAA requires regulated entities to implement security-incident procedures and audit controls capable of recording and examining activity in systems containing or using electronic protected health information. It does not require a particular SIEM, XDR, or MDR product.
SIEM, XDR, and MDR: Different Architectural Roles
SIEM as the Evidence and Correlation Plane
Security information and event management, or SIEM, collects and correlates telemetry across heterogeneous systems.
In healthcare, the SIEM may ingest events from:
- Identity and privileged-access platforms
- EHR audit systems
- FHIR servers and API gateways
- HL7 interface engines
- PACS and DICOM gateways
- Laboratory and pharmacy systems
- Firewalls, DNS, VPN, and NDR tools
- Cloud control planes
- Backup and virtualization platforms
- Endpoint security tools
The SIEM can become the primary evidence plane, but only when the organization controls log integrity, time synchronization, access, retention, parser versions, and evidence exports.
XDR as the Integrated Detection and Response Plane
Extended detection and response, or XDR, correlates security activity across supported endpoints, identities, email, cloud workloads, and applications.
Its primary architectural advantage is native response. Depending on the platform, XDR may:
- Isolate an endpoint
- Revoke an identity session
- Quarantine an email
- Disable an account
- Block an indicator
- Consolidate related alerts into one incident
XDR is generally strongest within its supported technology ecosystem.
It may not provide complete coverage for specialized clinical applications, legacy systems, medical devices, or acquired healthcare environments.
MDR as the Managed Operations Layer
Managed detection and response, or MDR, adds continuous monitoring, investigation, threat hunting, escalation, detection tuning, and authorized response.
The healthcare organization should retain control over:
- Clinical-impact decisions
- Downtime activation
- Risk acceptance
- Regulatory reporting
- Recovery authorization
- High-impact containment
An MDR provider that creates, receives, maintains, or transmits ePHI on behalf of a regulated healthcare organization may be acting as a business associate and require appropriate contractual safeguards.
Healthcare SOC Reference Architecture
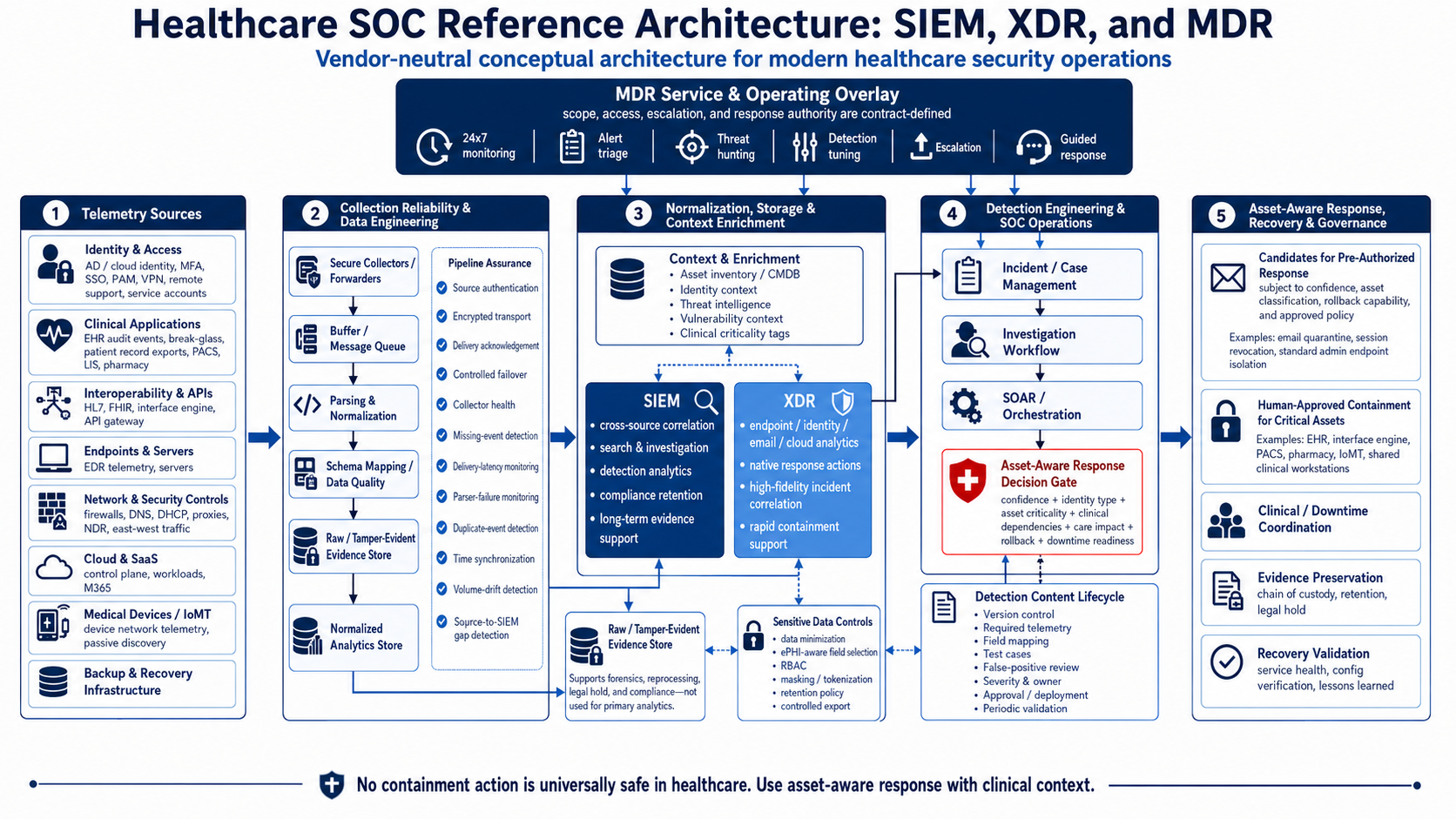
Disclaimer: This is a vendor-neutral conceptual reference architecture. Actual implementation must be tailored to the organization’s technology stack, clinical workflows, security risks, and response policies.
Layer 1: Telemetry Collection
Telemetry onboarding should follow attack paths and clinical risk instead of starting with the easiest connectors. Priority sources include:
Identity and Access
- Active Directory and cloud identity
- MFA and single sign-on
- Privileged-access management
- VPN and remote-support tools
- Service-account authentication
- Identity-policy changes
Clinical Applications
- EHR audit events
- Break-glass access
- Patient-record exports
- FHIR client activity
- HL7 route changes
- PACS administration
- Laboratory and pharmacy access
Infrastructure and Networks
- EDR and server telemetry
- Firewalls, DNS, DHCP, and proxies
- NDR and east-west traffic
- Hypervisors and backup systems
- Cloud control-plane events
- Medical-device network segments
HHS healthcare cybersecurity goals specifically identify centralized log collection, network segmentation, incident-response preparation, asset management, endpoint protection, and SOC capabilities as important healthcare security outcomes.
Layer 2: Collection Reliability and Data Quality
Collectors should support encrypted transport, source authentication, buffering, delivery acknowledgement, and controlled failover.
The SOC should continuously monitor:
- Missing events
- Delivery latency
- Parser failures
- Duplicate events
- Timestamp drift
- Unexpected volume changes
- Collector health
- Source-to-SIEM delivery gaps
A sudden absence of logs from an identity provider, EHR, backup platform, or domain controller should generate an alert.
Attackers may attempt to impair logging or security telemetry to reduce defender visibility.
Layer 3: Normalized Security Events
Original events should be preserved separately from normalized events.
The raw tier supports forensic validation and reprocessing. The normalized tier enables correlation across different products.
A normalized event should include identifiers that connect technical activity to healthcare operations.
{ "event_time": "2026-07-01T14:22:31Z", "ingest_time": "2026-07-01T14:22:36Z", "event_category": "application_activity", "event_action": "bulk_export", "event_outcome": "success", "user_id": "usr-28491", "user_type": "workforce", "source_ip": "198.51.100.24", "device_id": "ws-clinical-044", "application": "enterprise_ehr", "facility": "hospital-east", "records_accessed": 8421, "clinical_criticality": "high", "approved_workflow": false, "raw_event_reference": "evidence://ehr/2026/07/01/938211" }
This is an illustrative canonical event, not a normative OCSF payload.
OCSF can provide a vendor-neutral schema framework for cybersecurity events, but it remains agnostic to storage format, collection technology, and ETL implementation. Healthcare organizations must still engineer connectors, mappings, quality controls, and schema governance.
Logs may contain patient identifiers or other sensitive data. Collect only the fields required for approved detection, investigation, forensic, and compliance use cases.
Layer 4: Detection Engineering
XDR should handle high-fidelity detections within supported security domains. SIEM should handle cross-domain correlations involving clinical systems, identity, cloud, network, and infrastructure data.
High-value healthcare detections include:
- Risky authentication followed by bulk EHR export
- Privileged access followed by backup deletion
- Service-account activity from an unapproved host
- A new HL7 route or FHIR client registration
- Lateral movement toward PACS or pharmacy segments
- EDR tampering during file-encryption activity
- Break-glass access outside an expected care workflow
- New administrative access to an interface engine
Detection content should be version controlled and include its required telemetry, rule owner, false positives, severity, investigation procedure, test evidence, and response authority.
Illustrative Sigma Detection
title: Unapproved High-Volume EHR Record Export id: 17216f60-06a6-4bce-bbee-f05e61dba961 status: experimental logsource: category: application product: healthcare_ehr detection: export_activity: event_action: bulk_export event_outcome: success records_accessed|gte: 500 approved_accounts: user_id|expand: "%approved_bulk_export_accounts%" condition: export_activity and not approved_accounts falsepositives: - Approved health information management export - Authorized legal or regulatory disclosure - Scheduled analytics extraction level: high
Sigma is a structured YAML-based detection format. Numeric modifiers such as gte are supported, but backend support, field mappings, and log-source definitions must be validated locally.
This rule is intentionally incomplete. A production detection should also consider identity risk, export history, approved purpose, destination, time of day, facility, and peer-group baseline.
Layer 5: Asset-Aware Response
No containment action is universally safe in healthcare.
Response decisions should evaluate:
- Detection confidence
- Asset criticality
- Identity type
- Clinical dependencies
- Current care impact
- Rollback capability
- Redundant workflows
- Downtime readiness
Illustrative Response Guardrail
def containment_decision(incident, asset): if incident.confidence < 0.90: return "INVESTIGATE_ONLY" if asset.clinical_criticality in {"life_safety", "high"}: return "SECURITY_AND_CLINICAL_APPROVAL" if asset.type in { "ehr_server", "interface_engine", "medical_device", "pacs_gateway", "pharmacy_system" }: return "HUMAN_APPROVAL_REQUIRED" if not asset.rollback_tested: return "HUMAN_APPROVAL_REQUIRED" return "PREAUTHORIZED_CONTAINMENT"
This pseudocode demonstrates the decision model. It is not a complete SOAR playbook.
Lower-risk candidates for pre-authorized automation may include quarantining confirmed malicious email, revoking a suspicious cloud session, or isolating a standard administrative endpoint.
Actions affecting EHR servers, shared clinical workstations, interface engines, PACS, pharmacy systems, medical devices, or identity infrastructure should normally require human approval and, where applicable, downtime coordination.
3 Architecture Patterns
Pattern 1: SIEM-Centered with XDR Response
Best suited to health systems with multiple EHRs, clouds, hospitals, and security vendors.
The SIEM provides enterprise correlation and evidence retention. XDR supplies native endpoint, identity, email, and cloud response.
Pattern 2: XDR-Led with Selective SIEM Retention
Best suited to organizations standardized around one security ecosystem.
XDR performs primary detection and response. The SIEM retains selected clinical, infrastructure, compliance, and cross-vendor telemetry.
Pattern 3: Co-Managed SIEM and XDR with MDR
Best suited to organizations that own security platforms but need continuous monitoring, threat hunting, detection engineering, or incident support.
The MDR provider works within predefined authority boundaries. The healthcare organization retains clinical, regulatory, and recovery decisions.
Implementation Sequence
- Map clinical services, identities, applications, devices, interfaces, vendors, and network dependencies.
- Define a telemetry contract covering event types, schema, ownership, latency, retention, ePHI exposure, parser version, and health checks.
- Onboard identity, endpoints, remote access, email, backups, EHR audits, domain controllers, cloud platforms, and critical integrations first.
- Develop and test detections using representative events and controlled attack simulations.
- Classify response actions as pre-authorized, approval-based, emergency-only, or prohibited.
- Test collector outages, parser failures, ransomware activity, identity compromise, backup tampering, downtime escalation, rollback, and recovery validation.
NIST SP 800-61 Revision 3 integrates incident response across cybersecurity governance, identification, protection, detection, response, and recovery. Healthcare SOC modernization should therefore connect detection operations with resilience, continuity, and executive risk management.
Modernize Your Healthcare SOC With CapMinds Services
CapMinds helps healthcare organizations design and operationalize security architectures that protect ePHI while accounting for clinical availability and patient-safety requirements.
Our services include:
- Healthcare SOC architecture assessments
- SIEM, XDR, EDR, NDR, and SOAR integration
- EHR, HL7, FHIR, PACS, cloud, and identity telemetry onboarding
- Log normalization and parser engineering
- Healthcare detection engineering
- Clinical-safe response playbooks
- MDR operating-model design
- Medical-device security monitoring
- Ransomware and incident-response exercises
- HIPAA, HHS, and NIST-aligned security governance
- Security-platform optimization
- Recovery and response validation
- And more
A modern healthcare SOC must do more than generate alerts.
It must connect technical activity to clinical impact, preserve reliable evidence, coordinate safe containment, and support recovery without unnecessarily disrupting patient care.