The Complete Guide to Population Health Management for Healthcare Organizations

Population Health Management is changing the way healthcare organizations manage population health on a population level and, at the same time, manage the cost of care. PHM involves taking an overall view of caring for defined populations, using a proactive approach based on the best available data to effectively manage the health status of defined groups. To be able to effectively develop PHM programs, healthcare executives, clinicians, IT leaders, and policymakers need to understand the important elements involved in the concept of PHM, especially with the current transition to community wellness and value-based care.
This guide explains the key components of PHM. It demonstrates how to implement an efficient PHM Program using real-life examples and applications of the program. The resource also covers all main elements of PHM, such as Data Collection, Analysis, Coordinating Care, Patient Engagement, Preventive Health, & Health Equity. This resource teaches you to successfully utilize PHM to improve your outcomes, decrease costs, and create a healthier community.
What Is Population Health Management?
The Population Health Management is an approach that utilizes both data and coordination of care, and a variety of targeted interventions to enhance the health outcomes for certain populations. Unlike traditional medicine which reacts to illness as it occurs for each individual, the PHM’s objective is to monitor and manage the total population defined by it, therefore, preventing the occurrence of disease; managing the treatment of chronic disease; and reducing core area inequalities through the delivery of the right care at the correct time, etc., therefore enhancing every area of a population’s health.
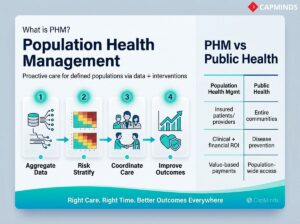
As an example, the way the PHM works is as follows: Find, collate, consult and analyse all client health data from many sources, using the analysis to determine which clients are at risk and where they might be deficient in their care; contact those clients and provide coordination of services from client health providers; contact clients regarding prevention of disease, treatment of chronic disease, etc.; provide education and/or provide assistance to eliminate social and cultural barriers to providing the proper level of care.
What’s the Difference Between PHM and Public Health? When comparing Population Health Management to Public Health, it is important to recognise that many aspects of PHM are similar to the broad community approach of Public Health for all people. In contrast, the focus of Population Health Management is the management of the health of those patients who are members of a health care delivery system or are in an insurance programme. The goal is typically to improve clinical outcomes and the financial performance of providers under value-based payment arrangements, rather than simply reducing costs for care.
PHM provides a bridge between traditionally separated clinical and non-clinical aspects of healthcare delivery systems by placing accountability on healthcare providers for the health outcomes of specific groups of individuals.
Why Population Health Management Matters
PHM is essential to the health care industry because it allows for improved quality, greater control over costs, and improved patient experiences, among numerous other benefits. Here are just a few of the major reasons that PHM plays such an essential role in health care today:
Improved Outcomes and Wellness
PHM prioritizes the provision of wellness-based, preventative health care over reactive sick care. When care is provided in this manner, individuals remain healthier as a result.
Coordinated actions will reduce complication rates related to chronic disease while allowing for health-related problems to be detected sooner. This will result in improved health for individuals, as well as overall community health.

Reduced Costs and Avoidable Utilization
Coordinating population health management activities will reduce the number of emergency department visits and hospitalizations experienced by your patient base. The health care costs for a small group of high-risk patients account for a large percentage of your health care budget.
About half of your healthcare expenditure will be attributed to the most severely ill 5% of patients and their care. PHM is targeted toward these high-risk patients by assisting healthcare providers in providing early intervention and monitoring of these patients to assist in preventing high-cost events.
- When healthcare providers effectively utilize PHM through their primary care leadership, they have successfully reduced hospitalizations and emergency department visits by nearly 96,000 and 167,000, respectively, for one calendar year.
- The financial impact of decreases in the number of crisis-related hospital visits and hospital admissions will create significant cost savings for both health systems and payers.
Higher Quality of Care
PHM initiatives have the primary goal of closing the existing gaps in the delivery of evidence-based medicine to patients. This means making sure every patient receives the preventive services, for example, for chronic diseases, on time. In value-based care programs, organizations that use PHM tools have noticed better quality metrics.
- One health system saw colorectal cancer screening rates increase by 3% for minority patients who were previously not screened using targeted PHM communications.
- These improvements in access to screenings create a direct pathway to improve the overall quality rankings and the patient outcomes for that entire system of care.
Enhanced Patient Experience
Another key principle of PHM is the engagement and satisfaction of the patients with their care. Care coordinators or digital outreach provide assistance and support for patients between routine visits.
When patients think that they are supported or recognized for their overall needs and concerns (feelings), they will be more likely to participate in their care process and maintain compliance with recommended treatments.
This leads to better experiences and trust. Coordinated care also reduces the frustration of repeated tests or having to repeat information to several providers.
Accountability in Value-Based Care
As healthcare payment moves from fee-for-service to value-based reimbursement, providers receive rewards for keeping populations healthy instead of merely treating illness.
- PHM is the mechanism that enables success in models like Accountable Care Organizations, capitated contracts, and shared savings programs.
- Healthcare executives and CIOs recognize that without robust PHM systems, organizations risk failing to meet quality and cost targets under these new models.
- In contrast, effective PHM can unlock financial incentives.
Addressing Health Equity
To eliminate health inequalities from healthcare, PHM customizes healthcare to provide services only to those individuals identified as being “at risk.” As examples, PHM examines clinical and social data to help identify underserved populations and provides targeted services for those groups.
- For instance, some PHM programs utilize medical interpreters/ambulatory interpreters near many patients with limited English proficiency.
- Additionally, some PHM programs partner with local food shelves to assist patients experiencing food insecurity.
- The outcome is fairer care delivery, ensuring that health results improve not only on average but also for every segment of the population. This idea is being recognized as the “fifth aim” in healthcare quality improvement.
Implementing an Effective Population Health Management System: Step-by-Step
To create an effective population health management strategy, you need to integrate various important aspects into one cohesive approach.
To do this successfully, it is important to look at what the various pieces of PHM consist of – from collecting data through to analysing that data for insight, all the way to taking action via Co-ordination of care and patient engagement.
The steps outlined here create a continuous cycle of improvement from the raw data collected through to a healthier group of patients/populations. Separate sections are provided for each component in the process.
1. Data Aggregation and Integration of Healthcare Data
The foundation of PHM is data. The ability to manage the health of a population necessitates your knowledge of who each patient is, what medical services he/she has received, and the potential risk factors associated with that person. The process of gathering and unifying multiple data points into a single dataset is known as Data Aggregation. A complete population health management program will include data from multiple sources, including:
- Electronic Health Records: This is the clinical information generated during an individual patient visit, including their medical history.
- Insurance Claims: This includes the patient’s diagnosis/procedure/prescriptions filled, and this may, in some cases, be the way you receive information regarding care provided outside your healthcare system.
- Pharmacy and Lab Systems: This data provides you with information about when the individual filled their prescriptions, received lab results, and imaging reports.
- Behavioral Health and Social Services: This includes data regarding the individual’s mental health and the community services/social determinants that the individual is utilizing.
- Connected Health Devices and Apps: The rise of wearable health devices, mobile apps connected to remote patient monitoring, and the growing availability of data from these devices and apps enrich your population’s health management database.
- Demographic and Socioeconomic Data: Data points including age, gender, language, race/ethnicity, income level, and geographic location are helpful in understanding the needs for, and disparities related to, social determinants of health.
Merging data from these disparate systems can be challenging from an IT perspective. Different EHR systems may not talk to each other, and data may come in various formats. Health CIOs and IT teams often use data warehouses or health information exchanges to aggregate data.
Modern PHM platforms utilize interoperability standards to consolidate data from disparate systems into a single location. The end product of this initiative will be the development of a ‘single source of truth’ about each patient as well as about the overall population of patients.
After aggregation has occurred, data is almost always cleaned and normalized so that accurate comparisons and analytics are possible. This extensive effort will reap huge benefits because healthcare leaders and care teams will have access to a complete view of the patient’s needs and the trends affecting their care.
Benefits of robust data aggregation include:
- Comprehensive View: Providers can see one patient’s data in the context of thousands of others, enabling more informed decisions. For instance, knowing how a patient’s lab result compares to similar patients can guide how aggressively to treat.
- Enhanced Data Quality: The combination of significant amounts of data results in improved accuracy of information. Spotting outliers or erroneous data points becomes simpler, and information missing from one dataset might be available in another.
- Reduces Administrative Burden: Clinicians and analysts have immediate access to all available data instead of having to compile multiple datasets manually. This availability saves both time and decreases the likelihood of error.
- Empowers Advanced Analytics: The combination of multiple datasets enables advanced analytics. Patterns that aren’t evident in isolated charts emerge when data is pooled.

2. Data Analytics and Insights for Population Health
With a rich, integrated dataset in hand, the next step is to derive meaningful insights through healthcare analytics. Data analytics in PHM encompasses a range of techniques, from basic reporting to advanced predictive modeling, all aimed at understanding the population’s health status and identifying where to intervene. Key analytics activities in PHM include:
Risk Scoring and Prediction
- Using algorithms, each patient can be assigned a risk score for outcomes like hospitalization or complications.
- These models consider clinical factors and sometimes social factors to predict who is most likely to have high costs or adverse events in the future.
- Predictive analytics allow care teams to focus on patients who need the most attention before they deteriorate.
Stratifying and Segmenting Populations
- Analytics tools segment the population into meaningful groups, for example, identifying all patients with uncontrolled diabetes, or seniors living alone, or children who missed vaccinations.
- Segmentation helps in tailoring interventions to each cohort’s needs.
Identifying Care Gaps
- A core use of PHM analytics is finding gaps in care, instances where a patient hasn’t received evidence-based care.
- For example, analytics might flag patients with diabetes who are overdue for an A1c test, or patients over 50 who haven’t had a colonoscopy.
- These care gap reports guide outreach efforts to ensure patients get recommended preventive and chronic care on time.
Population Health Dashboards
- PHM systems often feature dashboards that display key metrics: chronic disease control rates, hospital readmission rates, screening rates, etc.
- Executives and clinicians can monitor performance at a glance and drill down into areas of concern.
- High-level dashboards help leadership track progress toward goals like reducing ER visits or improving patient satisfaction.
Trend Analysis
- By examining data over time, analytics can show trends.
- Are hospitalizations increasing or decreasing this quarter?
- Is the average HbA1c for diabetics improving since a new program started?
- Trend analysis is crucial for evaluating the impact of PHM initiatives.
Social Determinant Insights
- Advanced PHM analytics incorporate social determinants of health data to identify how factors like poverty, housing, or transportation are affecting health outcomes.
- For instance, analytics might reveal that patients in a certain zip code have lower preventive screening rates, pointing to a potential access issue to address.
One powerful example of analytics in action comes from Allina Health. They used population health analytics to uncover disparities in colorectal cancer screening among specific minority groups. By drilling into the data, they discovered lower screening participation in these communities.
In response, Allina developed a program with home-based screening kits and culturally tailored education in patients’ native languages. The result was a 3% relative improvement in screening rates for those populations, a tangible outcomes gain driven by data insight and targeted action.
Analytics is also the engine behind evaluating PHM success. As interventions roll out, data is continuously analyzed to see if metrics improve, for example, did a new care coordination program reduce 30-day readmissions? Robust analytics infrastructure ensures organizations can measure outcomes and ROI for their PHM efforts, creating a feedback loop for continuous improvement.
3. Risk Stratification of Patient Populations
Risk stratification, which allocates risk teams to patients based on their health condition and anticipated care requirements, is a critical element of population health management. The analytics utilized in this process supply insight into the population that is at the highest risk of poor health and the need for the quickest and most comprehensive interventions.
How Risk Stratification Works
Using data on diagnoses, utilization history, socio-demographics, and sometimes special risk assessment tools, patients are stratified such that:
- High-Risk/Complex Patients make up a small portion of all patients, but these patients are usually those who have several chronic diseases and/or utilize a greater amount of healthcare services due to frequent hospitalizations.
- Rising-at-Risk Patients are a much larger group and represent those patients who are not currently critically ill but are likely to deteriorate unless they receive timely and appropriate health interventions.
- The majority are “low-risk” healthy or stable patients who need routine preventive care but not intensive management.
Often this is visualized as a risk pyramid: the sickest, costliest patients at the top (small in number but big impact), and the healthiest at the broad base. For example, an analysis might show 3-5% of your population is “high-risk” yet driving half of all costs. Those are the people a PHM program must identify and manage closely.
Why stratify?
Because it helps allocate resources efficiently. The limited number of care managers, outreach staff, and budget for healthcare organizations will affect how care is delivered.
Risk stratification prioritizes those patients at the highest risk for receiving the greatest level of service, moderate-risk patients receiving lower levels of service intervention, and low-risk patients receiving only automated preventive reminder messaging.
A tiered approach is critical to maximizing the impact of these interventions. In the implementation of risk stratification, some areas that may be referenced include:
- Chronic Disease and the Extent of Disease Severity: for example, having multiple comorbidities would indicate a higher risk level.
- Recent Utilization: Having more than two hospitalizations in the past six months would indicate a patient is unstable.
- Polypharmacy: Could indicate a high level of complexity.
- Social Determinants of Health: A patient living alone with limited assistance/ supports, low health literacy, or financial hardships would elevate a patient to a higher-risk category, as these conditions are associated with higher levels of negative health outcomes.
- Behavioural Health: Patients experiencing any underlying mental health and/or substance use disorder would indicate a higher risk categorization.
It’s important to note that risk stratification isn’t one-and-done; it should be a dynamic process. Patients can move between risk tiers as their health status changes.
For instance, someone might move from rising-risk to high-risk after a new diagnosis, or from high-risk down to moderate if a care plan stabilizes their condition.
Using Risk Stratification
After patients have been stratified, PHM programs can implement appropriate strategies for each stratification tier.
- High-Risk Patients: Typically placed in a high-intensity care management program where they receive services from a dedicated Nurse Care Manager, Care Team, or Care Manager in conjunction with regular visits for medication management, as well as follow-up after discharge from a hospital. Most ACOs have developed a method to track and triage patients from the top 5% highest risk patients to prevent future hospitalizations/complications.
- Rising Risk Patients: Assigned to either preventive coaching or disease management programs, they may qualify for preventive diabetes programs if they are pre-diabetic, or pulmonary rehabilitation and smoking cessation if they are at risk for experiencing severe COPD exacerbations.
- Low Risk Patients: Primarily managed through organization-wide prevention strategies, i.e., reminders about their annual wellness exams, immunizations, cancer screening, and using digital resources such as patient portals for self-management; also, they likely only need access to their primary care doctor’s office for routine follow-up care.
Using risk stratification allows providers to deliver targeted care coordination to give the most benefit from the resources used. Balancing this process accurately means not missing patients who may be at risk of hospital admission tomorrow by ignoring them, but at the same time not giving every patient a high-intensity intervention.
4. Care Coordination and Care Management
The next very important part of the process is Care Coordination, which organizes all health care activities within or across all providers and locations. This means to help the patient navigate the health care system to make sure they receive the same type of care throughout their journey through the health care system, for example, through a hospital stay.
Traditionally, when patients enter the health care system, their care is often fragmented. Patients see many different specialists, have a hospital stay, and go to a rehabilitation facility, but there may be little or no communication between providers. Care coordination provides a central focus for coordinating a patient’s journey. Key elements include:
Care Management Teams
To enhance the care experience for high-risk patients, many Population Health Management Programs employ Care Managers. A care manager acts as a single point of contact that ensures coordination and overall management of the patient’s care plan. Care Managers are responsible for coordinating appointments, ensuring that all follow-up appointments are completed, reconciling medication lists, and communicating with all providers involved in the care of the patient.
Interdisciplinary Collaboration
Many complex patients require multiple types of interdisciplinary input from their Primary Care Physician, Specialties, Pharmacy, Mental Health Providers, and Community Services.
This collaboration is facilitated through regular team huddles and case conferences, where the various medical professionals involved have the opportunity to discuss the goals of the patients and collectively arrive at a treatment plan for that patient. For example, during the weekly Care Coordination Meeting, the top 10 highest-risk patients will be reviewed and have a current course of action established for them.
Transitions of Care
Coordinated care from a primary health management team will often focus on the patient’s transition from hospital discharge back home. PHM teams will coordinate care for patients post-hospital discharge through communication with and prompting primary care providers to schedule their first appointment within seven days of discharge, sending all medical providers a copy of the hospital discharge summary, and calling the patient at home after discharge to ensure understanding of medication and discharge instructions. All of these activities are designed to eliminate the black hole that patients frequently enter after being discharged from a hospital, thereby significantly reducing the number of readmissions to hospitals.
Patient Navigation
One of the key roles of care coordinators is to serve as navigators for patients to help them navigate barriers to healthcare access and utilization within the healthcare system. Care coordinators assist patients in scheduling their specialty appointments and arranging for transportation to those appointments. In addition to coordinating the patient’s care, the navigator works closely with the patient to ensure that he/she is not failing to receive necessary care due to logistical issues.
Single Care Plan
Ideally, the patient has one consolidated care plan that all team members can reference. This care plan includes the patient’s health goals, the interventions planned (e.g., home visits by a nurse or enrollment in a nutrition program), and who is responsible for each aspect. It keeps everyone on the same page and the patient at the center of decisions.
Care coordination example
Imagine a 68-year-old patient with heart failure, diabetes, and depression, a classic high-risk profile. In a PHM program, this patient might have a nurse care manager who calls weekly to monitor weight and symptoms, coordinates with a cardiologist for medication adjustments, connects the patient with a diabetes educator, and arranges counseling for depression. When the patient was recently hospitalized for breathing issues, the care manager ensured a follow-up home visit was done, and a dietitian reviewed their low-salt diet. Thanks to these coordination efforts, the patient’s conditions are stable, and they haven’t been back to the hospital in months.
For healthcare executives, care coordination is where the “rubber meets the road” in PHM. It’s resource-intensive, but it directly impacts outcomes and costs by avoiding duplication, preventing errors, and keeping patients engaged in appropriate care. In fact, care coordination programs are proven to reduce avoidable admissions and ER visits, especially for patients with multiple chronic conditions.
A well-coordinated system also improves provider satisfaction: clinicians can work at “top of license” when care managers handle a lot of the outreach and follow-through, and everyone has better information to make decisions. It addresses the frustration providers feel when they don’t know what other treatments the patient received elsewhere.
5. Patient Engagement and Empowerment
An often-repeated saying in healthcare is: “The patient is the most important member of the care team.” Patient engagement is a core component of population health management because even the best care plan on paper won’t succeed if patients aren’t on board. Engaged patients are active participants in their health; they understand their conditions, adhere to treatments, and make informed decisions. PHM initiatives devote significant effort to empowering patients and their families in the care process.
Key strategies for patient engagement in PHM include:
Education and Health Literacy
Providing patients with easy-to-understand information about their conditions and treatments. This might involve one-on-one counseling, group workshops, or printed and digital materials. The goal is to improve health literacy so patients comprehend why certain actions are crucial. Many PHM programs employ health coaches or educators to work with targeted groups.
Personalized Communication
Moving beyond generic reminders, PHM uses personalized outreach. For example, sending tailored messages via patient portals, text, or phone calls: “John, according to our records, you’re due for a blood pressure check. Let’s schedule that so we can keep you on track.” Personalization shows patients that their care team is following their progress. It’s also important to communicate in the patient’s preferred language and mode; some may engage better via a phone call from a nurse, others via a mobile app notification.
Digital Engagement Tools
Technology greatly enables patient engagement. Patient portals allow individuals to view their lab results, message their providers, and access educational content. Many PHM programs push the use of portals or apps to facilitate continuous engagement. For instance, a portal might send alerts: “It’s time to schedule your annual wellness visit” or “New message from your care coach.” Additionally, remote monitoring devices keep patients involved daily and provide real-time data to the care team. Gamification and goal-tracking features in apps can motivate patients to hit targets.
Shared Decision-Making
Engaged patients are involved in choosing their care path. PHM encourages providers to practice shared decision-making, where the clinician presents options, and the patient’s values and preferences guide the plan. For example, for a patient with chronic knee pain, the care team might discuss physical therapy vs. surgery vs. a weight loss plan, and the patient’s lifestyle and preferences will shape the strategy. When patients help design their care plan, they are more likely to commit to it.
Support Networks and Peer Engagement
Some population health programs facilitate support groups or peer mentors, especially for chronic conditions like diabetes, heart disease, or cancer survivorship. Peer support can significantly boost engagement; it helps patients feel they’re not alone and lets them learn coping strategies from others who have “been there.” For instance, a PHM initiative might set up a community forum (online or in-person) for patients managing hypertension to share tips and encouragement.
Addressing Barriers to Engagement
A critical part of engagement is identifying why a patient may not be following through. Is it a cost? Transportation? Cultural beliefs? In PHM, care teams frequently assess these barriers during interactions. Solutions can include connecting patients with financial assistance, arranging rides, or enlisting community health workers who have cultural and language concordance to build trust. Overcoming these barriers is essential for true engagement.
Why it matters
Studies have shown that better patient engagement leads to better outcomes, for example, higher medication adherence, improved chronic disease control, and lower hospitalization rates. From a business perspective, engaged patients also tend to utilize preventive services more and report higher satisfaction. For population health, engagement at scale means a healthier population that self-manages effectively and uses healthcare resources more appropriately.
Patient Engagement Example
Consider a scenario in a PHM program for patients with hypertension. Instead of just telling the patient “take your blood pressure pills,” the program might issue each patient a digital BP cuff and a smartphone app. Patients are trained how to use it and record daily readings.
The app provides feedback. A nurse navigator monitors the data and reaches out if readings are consistently high or if the patient stops checking. Meanwhile, monthly virtual group sessions are held where patients can talk about diet challenges or share successes. Over time, this multi-faceted engagement approach leads to improved blood pressure control across the population, because patients feel accountable and supported daily, not just when they happen to see their doctor.
Key Patient Engagement Tools in PHM:
- Patient portal systems
- Mobile health apps
- Automated call or text reminder systems
- Telehealth visits and remote monitoring
- Educational workshops/webinars
- Patient advisory councils (involving patients in designing the PHM program itself)
6. Preventive Care and Wellness Programs
Preventive care is the heart of any population health strategy. It’s far more effective (and cost-efficient) to prevent illness or catch it early than to treat advanced disease. PHM puts heavy emphasis on wellness, screenings, and early interventions to keep the population healthy. This component focuses on shifting the healthcare mindset from reactive sick care to proactive health maintenance.
Key aspects of preventive care in PHM include:
Routine Screenings
Ensuring that patients receive age and risk-appropriate screenings is a fundamental PHM activity. This includes screenings for cancer, chronic conditions, and other tests like osteoporosis scans. PHM systems track which patients are due for what and trigger outreach.
- For example, if a 52-year-old hasn’t had a colorectal cancer screening, the system will flag it so the care team can remind and arrange it.
- Over a population, these efforts lead to higher screening rates, which means earlier detection of diseases when they are more treatable.
Immunizations
Vaccination campaigns fall under PHM as well, from childhood immunizations to annual flu shots to vaccines for older adults. High immunization coverage in a population can prevent outbreaks and protect vulnerable patients. PHM programs often coordinate flu shot clinics or mobile vaccination drives, and use data to identify pockets of under-vaccination to target with education.
Wellness Visits and Risk Assessments
Many PHM models incorporate annual wellness visits or health risk assessments, where patients fill out questionnaires about lifestyle, nutrition, mental health, etc. These serve as preventive touchpoints to spot issues like depression, fall risk, or obesity early. The care team can then intervene with appropriate referrals.
Lifestyle and Behavioral Programs
Preventive care isn’t just about medical tests; it’s also about promoting healthy lifestyles. PHM initiatives may include wellness programs such as smoking cessation clinics, weight management classes, exercise programs, stress management and mindfulness workshops, and so on.
For instance, a PHM program might have a “Diabetes Prevention Program” targeted at pre-diabetic individuals, focusing on diet and exercise coaching to prevent progression to diabetes. Another example is a maternity care program that provides prenatal education to expectant mothers to improve birth outcomes.
Preventive Outreach
A hallmark of PHM is outreach before patients feel sick. This might involve sending reminders for regular check-ups, reaching out to patients who haven’t been seen in over a year, or using community health workers to visit patients in the community with preventive education.
Preventive outreach acknowledges that many people “don’t know what they don’t know”, by nudging them to seek preventive services, PHM reduces the number of patients who present with advanced illness because they never got that earlier intervention.
Tracking Population Health Metrics
At a macro level, PHM programs track metrics like vaccination rates, percentage of patients with controlled blood pressure, obesity rates, smoking rates, etc., across the population.
- Improvements in these metrics over time demonstrate success in preventive care efforts.
- For example, increasing the percentage of hypertensive patients whose blood pressure is controlled from 60% to 75% in a year would be a big population health win, likely reflecting effective medication management and patient lifestyle changes orchestrated by PHM.
It’s worth noting that preventive care yields returns both in health outcomes and financially. By catching issues upstream, you avoid expensive downstream treatments.
- For instance, controlling diabetes can prevent costly hospitalizations for heart attacks, strokes, or kidney failure.
- Regular cancer screenings can catch cancers at an earlier stage, where treatment is less invasive and more successful.
- These avoided costs are a key part of the business case for PHM, especially in capitated or shared-savings environments.
- Preventing a $50,000 hospitalization with a $200 intervention is a clear win.
Despite the known benefits, millions of people do not get recommended preventive services due to barriers like cost, access, or lack of awareness.
Population health managers work to reduce these barriers. This may involve community outreach programs, mobile clinics that bring services to underserved areas, partnerships with employers or churches to promote wellness, and policy advocacy.
7. Addressing Health Equity and Social Determinants of Health
No comprehensive population health strategy is complete without deliberately tackling health equity, ensuring that all segments of the population have a fair and just opportunity to achieve optimal health.
Health equity in PHM means proactively identifying and addressing the social, economic, and environmental factors that cause certain groups to suffer worse health outcomes than others. These factors, often referred to as Social Determinants of Health, include things like income, education, housing, access to food, transportation, discrimination, and more.
In a population, it’s common to find disparities: for example, low-income or minority communities might have higher rates of chronic disease and lower life expectancy. PHM uses data to shine a light on these inequities and then works to close the gaps.
Approaches to integrate health equity in PHM:
Data Stratification by Demographics
When analyzing population data, PHM teams stratify outcomes by race/ethnicity, gender, geography, etc. This can uncover hidden disparities. For instance, your overall diabetes control rate might look okay, but stratifying may show that control rates are much lower in a specific neighborhood or ethnic group. Identifying such gaps is the first step to addressing them.
Culturally Tailored Interventions
To effectively reach diverse groups, interventions should be culturally and linguistically appropriate.
- This could mean providing health coaches who speak the patient’s primary language, using community health workers from the same community as liaisons, or adapting educational materials to be culturally relevant.
- In the earlier example, Allina Health improved colorectal screening rates by using culturally sensitive education materials in patients’ primary languages, which specifically tackled a disparity in screening uptake.
Community Partnerships
PHM programs often partner with community organizations, such as local nonprofits, public health departments, faith-based organizations, schools, and social service agencies, to address upstream determinants of health.
For example, if a lack of healthy food is impacting a population, a PHM initiative might work with local food banks or create a “Food Rx” program where patients get vouchers for fruits and vegetables. If transportation is a barrier, partnerships with ride-share companies or community vans can be established to bring patients to clinics.
Social Needs Screening and Navigation
Many healthcare providers now incorporate SDOH screenings into patient visits or outreach calls. When a patient screens positive for a need, the PHM program has a process to connect them to resources.
- For instance, a positive screen for food insecurity might trigger a referral to a community food pantry or enrollment in a meals program.
- Large health systems sometimes employ dedicated social workers or patient navigators who specialize in connecting patients with community resources.
- By addressing these social needs, PHM helps remove barriers that might otherwise derail a patient’s health improvement.
Equity Metrics and Goals
Progressive organizations set specific health equity goals as part of their PHM KPIs. For example, a goal might be to reduce the gap in hypertension control between white and Black patients by X% in two years, or to ensure that colorectal screening rates reach at least 80% in all ZIP codes the system serves.
By making equity an explicit goal, the so-called “Quintuple Aim”, adding equity to the traditional aims, leadership signals its importance, and resources can be allocated to these efforts accordingly.
Workforce Diversity and Training
Ensuring the care team itself is trained in cultural competency and representative of the community can improve equity. PHM programs may include staff training on implicit bias, hiring bilingual staff for areas with language needs, or engaging community members in advisory boards to guide program design.
- Beyond the moral imperative, focusing on health equity can improve overall population outcomes.
- Often, by raising the floor, the entire population’s health metrics improve.
- From a cost perspective, health disparities are expensive: unmanaged chronic conditions in underserved groups lead to preventable ER visits and hospitalizations.
- By investing in equity, for example, better managing chronic disease in a low-income neighborhood, you can avoid those downstream costs.
- One ACO example showed that targeted interventions in underserved communities contributed to large savings and better outcomes.
A healthcare network observed that its asthma hospitalization rates were significantly higher for children in certain urban neighborhoods. Investigation revealed substandard housing and a lack of access to primary care as contributors.
In response, the PHM program partnered with the city’s public health and housing department to launch an “Asthma Safe Homes” project, providing home inspections and remediation.
They also set up mobile clinics in those neighborhoods for easier access to asthma check-ups and medications. Over time, asthma control improved, and pediatric asthma admissions fell in those areas. This is PHM addressing not just the medical side but the social/environmental side of health.
Technology and Tools Supporting Population Health Management
Implementing PHM at scale would be near-impossible without robust technology. In modern healthcare, data volume is immense, and workflows are complex; technology solutions are the enablers that turn PHM strategies into day-to-day operations. Key technologies and tools that drive successful PHM include:
Population Health Management Software Platforms
These dedicated systems aggregate data from various sources, provide analytics dashboards, and often include care management workflow tools. They act as a nerve center for PHM activities, allowing teams to track population metrics, stratify risk, document care plans, and monitor interventions.
Many PHM platforms integrate with electronic health records but provide a population-level view rather than just an individual patient view. For example, a PHM platform may generate a list of all diabetic patients with A1c > 9 and assign them to care managers for outreach, tracking that outreach to closure.
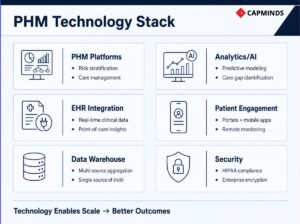
Electronic Health Records Integration
While an EHR alone isn’t sufficient for PHM, a tight integration between PHM tools and EHR is ideal. This means data flows both ways: the PHM system feeds insights into the EHR for the clinician to see at the point of care, and the EHR feeds real-time clinical data back to the PHM analytics. Some EHR vendors offer population health modules, but many organizations use third-party PHM solutions that connect to the EHR. The integration ensures that frontline providers have actionable population health information during visits, and PHM teams have up-to-date clinical inputs.
Related: The Role of EHR-HIE Connectivity in Population Health Management
Data Warehouses and Interoperability Solutions
On the backend, a lot of tech is about getting the data together. Health Information Exchanges, data warehouses, or interoperability platforms are deployed to aggregate and normalize data from multiple EHRs and systems. Interoperability remains a challenge in healthcare; many EHRs are siloed. Investing in this layer is critical so that PHM analytics aren’t limited to one source.
As noted, poor interoperability can hamper PHM efforts. Thus, many organizations partner with vendors or HIEs specifically to solve the data sharing problem, allowing a unified patient record across providers.
Analytics and Business Intelligence Tools
Under the hood, PHM uses analytics engines.
- Some are built into PHM platforms, but organizations may also leverage general BI tools or data science tools for custom analysis.
- Advanced analytics like predictive modeling might use machine learning platforms.
- AI and predictive analytics are emerging trends in PHM, for instance, using AI to predict which patients are at risk of medication non-adherence or who might benefit from palliative care referral.
- As PHM data grows, these tools become more powerful in finding patterns.
- Future-forward organizations are exploring artificial intelligence to enhance risk predictions and personalize interventions.
Patient Engagement Technology
On the patient side, telehealth platforms, mobile apps, and remote monitoring devices are increasingly part of PHM tech infrastructure. Telehealth expands access.
Mobile apps and portals were discussed earlier; they keep patients connected. Remote monitoring tools feed data into the system, giving care teams continuous visibility into patients’ health status between visits. PHM programs often create “digital front doors” for patients to engage, making care more accessible and timely.
Automation and Workflow Tools
Handling a population means automating repetitive tasks where possible, so staff can focus on the human-touch aspects. PHM platforms often include automation such as auto-generated patient lists for outreach, automatic assignment of tasks, and automated patient communications. This improves efficiency and ensures no patient falls through the cracks due to human oversight.
Security and Privacy Tech
Managing population data also means dealing with large-scale sensitive information. PHM implementations must include
- Strong cybersecurity measures,
- Patient consent management, and
- Compliance with regulations like HIPAA.
Data is often stored in cloud environments, which brings advantages in scalability and analytic power, but requires vigilant security protocols. For healthcare CIOs and CTOs, choosing the right tech stack for PHM is a major decision. Some opt for an all-in-one vendor solution; others build a best-of-breed ecosystem where an analytics platform, a separate care management app, and custom integrations all work together. Regardless, the technology should align with the organization’s workflow and goals.
User-friendliness is key; if care managers or clinicians find the software cumbersome, they won’t use it effectively. The best PHM tools integrate seamlessly into clinical workflows.
Importantly, technology is an enabler, not a silver bullet. As one industry saying goes, “A fool with a tool is still a fool.” Successful PHM requires not just tech, but also people and process changes. However, without modern tech, PHM at scale would be prohibitively labor-intensive and data-blind. With the right tools, a single care manager can track and coordinate care for hundreds of patients, something not feasible using manual methods.
- A medium-sized health system implemented a new PHM analytics platform integrated with their EHR.
- Almost immediately, they identified over a thousand patients overdue for colorectal cancer screening who otherwise might have been missed.
- They set up an automated outreach campaign through the platform, which sent texts and letters, and then tracked responses.
- Within 6 months, screening rates jumped significantly, catching several early cancers in the process.
- This is a clear example of how technology enabled a lifesaving preventive intervention at the population level, which manual efforts alone likely wouldn’t have achieved as efficiently.
Challenges and Risks in Population Health Management
Implementing population health management is a complex undertaking, and it’s not without its challenges. Being aware of these challenges can help organizations plan better and find strategies to overcome them.
Here are some common challenges and risks in PHM, along with brief notes on how to address them:
Data Integration and Quality Issues
Healthcare data comes from many sources and often in incompatible formats. Interoperability hurdles and data silos can complicate building a complete view of patients. Additionally, data may be incomplete or error-prone. Invest in robust data integration platforms and standards to connect systems. Employ data governance and cleaning processes to improve data quality over time.
Partnering with HIEs or using middleware solutions can also help bridge gaps. Ensuring data integrity is foundational; analytics are only as good as the data fed in.
Engaging Diverse Patient Populations
Populations are not monolithic; engaging patients from different cultural, linguistic, and socio-economic backgrounds can be challenging. What works for one group might not work for another. There can be language barriers, health literacy issues, and trust issues, especially in communities historically underserved.
Use tailored, culturally competent communication. Provide materials in multiple languages; hire staff from the community to serve as liaisons. Utilize multiple outreach channels to see what resonates. Building trust takes time; partnering with community leaders can help endorse the program.
Provider and Staff Buy-In
PHM often requires changes in workflow. Some providers may resist, seeing it as extra work or “not how I’m used to doing things.” There can be a learning curve with new tools.
Change management is crucial; involve providers early in planning, show them data on how PHM can reduce their workload long-term. Provide training and perhaps incentives or recognition for providers who excel in PHM metrics. Emphasize that PHM helps them provide better care. Leadership should champion PHM as core to the mission.
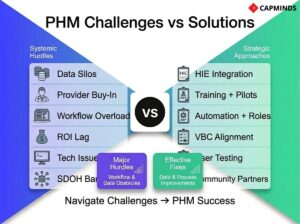
Workflow Integration
Related to buy-in, integrating PHM tasks into daily routines is challenging. Care teams might feel overwhelmed if PHM activities are just added on top of normal duties.
- Clearly define roles,
- Often, new roles like population health managers or analysts can take on the heavy data work, and
- Care coordinators handle many patient contacts, freeing physicians to focus on in-person care.
Use automation to streamline tasks. Start with pilot programs to refine workflows on a small scale, then scale up once bugs are ironed out.
Financial and ROI Concerns
Standing up a PHM program requires investment in technology, staff, and time. The return on investment might take a few years to materialize.
For organizations still paid largely fee-for-service, PHM can paradoxically reduce short-term revenue by cutting hospital admissions or procedures. This conflicting incentive can be a barrier.
- Align PHM efforts with value-based payment as much as possible.
- If you’re in fee-for-service, focus PHM on areas that also reduce the cost of providing care or improve efficiency.
- Use grant funding or partnerships to offset initial costs.
- It’s also important to track and tout early wins, e.g., if PHM prevented X admissions, saving Y dollars, share that data to build internal support.
- Long-term, as payers move to value-based contracts, PHM readiness will pay off, but bridging the short-term gap is a consideration.
Technology Challenges
Choosing the wrong platform, or dealing with IT glitches, can derail PHM. Systems that don’t talk to each other, or user-unfriendly interfaces, can frustrate staff. Additionally, concerns around data privacy and security are heightened when aggregating so much data; a breach or HIPAA violation is a significant risk.
Thoroughly vet technology solutions with input from end-users. Start with pilot tests. Ensure strong IT support and training. Implement strict security protocols and have a robust compliance framework in place. Regularly review and update data use agreements and patient consent where applicable, especially if using data for advanced analytics.
Addressing Social Determinants is Hard
It’s one thing to identify that a patient needs housing; it’s another to actually secure housing for them. Many PHM programs find limitations in what healthcare alone can do about social issues. Community resources might be lacking or stretched thin.
- Set realistic scopes; healthcare organizations should partner and facilitate rather than shoulder everything.
- Advocate for policy changes when systemic issues are beyond your reach.
- Also, be creative: some health systems are investing in affordable housing or legal aid for patients, recognizing the ROI in health outcomes.
These challenges are significant but not insurmountable. They underscore that PHM is as much a change management and systems engineering project as it is a clinical one. Organizations that succeed often do so by starting small, learning, and scaling up, all while maintaining flexibility to adjust strategies.
In fact, many best practices in PHM today come from early lessons learned in pilot programs that faced these hurdles. The key is to anticipate the challenges, measure progress, and continuously improve. For example, if initial patient outreach didn’t yield great responses, experiment with a different approach or channel. If providers are overwhelmed, adjust workloads or add support staff.
Ultimately, the reward, improved population health and more sustainable healthcare delivery, justifies navigating these challenges. It’s encouraging that each year, as PHM knowledge matures, there are more tools and success stories to draw upon to mitigate these risks.
Population Health Management Systems vs. EHR: What’s the Difference?
It’s common to wonder how a Population Health Management system differs from the traditional Electronic Health Record that clinicians use every day.
Both deal with patient data, but they serve different purposes in a healthcare organization. The table below highlights key differences between PHM systems and EHRs:
| Aspect | Population Health Management System | Electronic Health Record |
| Primary Focus | Population-Level Health: Manages health outcomes of groups of patients. Emphasizes trends, risk patterns, and proactive interventions across a defined population. | Individual Patient Care: Manages each patient’s medical record and care episodes. Focuses on documentation and treatment of the individual. |
| Scope of Data | Aggregated, Multi-Source Data: Integrates data from multiple sources to get a comprehensive view of patient populations. Often includes non-clinical data. | Single-Source Clinical Data: Contains detailed clinical information entered during encounters within one health system or practice. Primarily clinical data from that provider’s perspective, with limited external data. |
| Functionality | Analytics and Care Management: Provides tools for risk stratification, care gap identification, population analytics, and care coordination workflows. It can generate population dashboards and manage outreach tasks. Designed to support value-based care programs and team-based interventions. | Clinical Documentation and Transactional: Optimized for recording patient encounters, ordering tests, prescribing medications, and billing. EHRs excel at one-on-one clinical documentation and immediate patient care needs, but have limited built-in population analysis. Some have add-on modules for reports, but not as extensive as PHM systems. |
| Care Approach | Proactive & Preventive: Triggers actions such as reminders for preventive services, alerts for high-risk patients, and tracking of chronic disease metrics across many patients. The mindset is anticipating needs and outreaching to patients who aren’t in the office. | Reactive & Episodic: Generally used when a patient comes in for a visit or contacts the healthcare system. The focus is on treating the issue at hand. Preventive care reminders in EHR exist, but if the patient isn’t present, the EHR by itself doesn’t reach out. |
| Users | Population Health Teams and Analysts, plus Care Coordinators and sometimes Clinicians: PHM software is often used by a specialized team who identify where interventions are needed. Care coordinators use it to track outreach. Clinicians may interface with PHM insights via alerts or reports, but might not be primary users of the PHM interface daily. | Clinicians and Care Staff: EHR is used by doctors, nurses, therapists, etc., as the primary tool during patient visits. It’s also used by billing and coding staff, schedulers, etc. It’s the day-to-day system for delivering care and documenting it. |
| Interoperability | Built for Connectivity: Good PHM solutions are designed to pull and push data across systems. They often sit on top of multiple EHRs and data feeds. As such, they focus on data integration to achieve a unified patient record across settings. | Often Siloed (but improving): Traditional EHRs have had limited interoperability. An EHR mainly contains data entered in that system, and sharing with other systems has historically been challenging. |
| Value-Based Care Support | Core Purpose: PHM exists largely to enable value-based care. For example, tracking metrics for ACOs, managing chronic care management programs, and ensuring quality measures are met across the board. It’s aligned with population-level outcomes and cost reduction. | Secondary/Not Explicit: EHRs were originally designed for fee-for-service record-keeping. While they now include quality measure reports and some care coordination tools, they are not inherently built to manage financial risk or population metrics. Many organizations find EHRs insufficient alone for managing value-based programs, which is why PHM software is added. |
Use Cases and Examples of Population Health Management in Action
To bring all these concepts together, let’s look at some real-world use cases and examples where population health management strategies have made a tangible impact. These scenarios illustrate how PHM is applied in different settings and for different goals:
1. Managing Chronic Disease at a Health System
A large health system noticed that its patients with diabetes had suboptimal control, many had high HbA1c levels, and diabetes-related ER visits were frequent.
Using PHM analytics, the system identified 500 high-risk diabetic patients across its primary care clinics. They launched a PHM-driven Diabetes Care Program:
- Each patient was assigned a nurse care manager who checked in monthly, ensured they attended eye exams and foot exams, and coordinated any specialist referrals.
- Patients received education on diet, were connected with affordable healthy meal programs if food insecurity was noted, and those with financial barriers were enrolled in insulin assistance programs.
- Over a year, the population’s average HbA1c dropped by 1.5 points, ER visits for hypoglycemia/hyperglycemia dropped by 30%, and overall diabetes compliance metrics rose dramatically.
Better patient health and cost savings from avoided acute episodes. One patient story from this program was a man who, through regular calls, admitted he was cutting insulin doses due to cost; the care manager got him into an assistance program, potentially averting a dangerous complication.
This illustrates PHM’s power in chronic disease management: data identified who needed help, and coordinated care ensured they got it.
2. Reducing Hospital Readmissions through Transitional Care
An Accountable Care Organization focusing on Medicare patients implemented a PHM-based transitional care management initiative. They found that heart failure and pneumonia patients were frequently bouncing back to the hospital within 30 days. The PHM approach:
- A care transition nurse sees each of these patients before discharge,
- Schedules a home visit and a primary care follow-up within a week, and
- Make sure they go home with the necessary medications and understanding of symptoms to watch.
The PHM platform tracked all discharged patients and flagged any who missed follow-ups, prompting a call. Additionally, high-risk patients got remote scales and daily check-in calls. Over a year, the ACO’s 30-day readmission rate for those conditions dropped from 18% to 10%. This not only meant better patient outcomes but also significant savings and higher shared savings bonuses for the ACO.
ACO saved millions; as reported by Aledade, robust primary care and follow-up prevented tens of thousands of hospitalizations and ER visits, contributing to over $1 billion in Medicare savings in 2024.
3. Preventive Screening Outreach by a Health Insurer
A regional health insurance plan used PHM analytics to improve preventive care among its members. Data showed that colorectal cancer screening rates were only ~50% for eligible members, with even lower rates in certain minority groups.
The insurer’s PHM team worked with local clinics to identify patients overdue for screening. They launched a multi-faceted outreach: mailed easy at-home stool test kits to thousands of members, with instructions in English and Spanish and a helpline.
They also provided a $25 gift card incentive for completing the screening. For communities with language barriers, they partnered with community health workers to follow up in person and educate.
- As highlighted earlier, one health system in this effort saw a 3% relative increase in screening rates among previously under-screened groups, moving the needle on an important preventive metric.
- Across the insurer’s population, overall screening rates rose to 65%.
Several early-stage cancers and many polyps were detected that would have otherwise been missed. This example underscores how PHM initiatives by payers can improve public health outcomes.
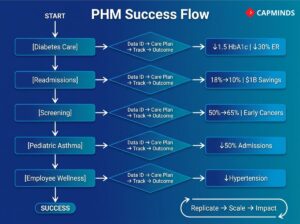
4. Addressing Social Determinants in an Urban Clinic Network
A network of community clinics serving an urban low-income population used PHM to tackle high pediatric asthma rates. They discovered that children from certain housing complexes had disproportionately more ER visits for asthma. A PHM approach revealed social factors at play; those buildings had mold and pest issues exacerbating asthma, and families had limited access to primary care.
The clinic network secured a grant and partnered with the city’s housing authority:
- They set up community asthma classes for parents,
- Provided free vacuum cleaners and mattress covers, and
- Had community health workers do home visits to educate about triggers.
Simultaneously, they extended clinic hours and ensured every asthma patient had an action plan and proper inhalers. They even worked with housing officials to improve living conditions. Within two years, asthma-related hospitalizations in that population dropped by 50%.
Children missed fewer school days, families had fewer emergency crises, and the overall cost of asthma care fell. This case shows PHM’s role in health equity, by identifying an at-risk population and coordinating beyond clinic walls, disparities in outcomes were reduced.
5. Employer Population Health Program
Population health principles also apply to employer or insurer wellness programs. Consider a large employer that self-insures its health plan. They used PHM analytics on their employee health data and found rising rates of hypertension and pre-diabetes among middle-aged staff, which could lead to costly claims down the road. They launched an employee wellness PHM initiative:
- Free on-site screenings,
- A digital app for weight loss challenges, and
- Health coaching for those at risk.
They even changed cafeteria offerings to healthier options. After 18 months, the number of employees with uncontrolled hypertension decreased significantly, and those who participated in coaching lost an average of 10 pounds. The company saw its healthcare costs stabilize and even decrease slightly, bucking national trends.
A healthier workforce with lower healthcare utilization is a win for both employees and the employer. This demonstrates PHM’s adaptability outside traditional clinical settings.
These examples highlight several key takeaways about PHM in action:
- PHM can be applied in various contexts, such as health systems, ACOs, insurers, community programs, and workplaces, with the common theme of proactive, data-driven intervention.
- Success often involves measurable improvements: lower hospital/ER utilization, better chronic disease metrics, higher screening rates, improved patient satisfaction, cost savings, etc. Always track and celebrate these to maintain momentum.
- PHM initiatives frequently require collaboration between different healthcare providers, between healthcare and community organizations, or between payers and providers. Breaking down silos is both a challenge and a requirement.
- Patient stories often illustrate the impact: whether it’s a patient avoiding a complication because someone cared to call them, or a community benefiting from targeted resources, PHM ultimately is about making health care more personalized and effective, even at scale.
By studying and replicating successful use cases and also learning from challenges they faced, healthcare organizations can refine their own PHM strategies. The evidence is increasingly clear that when done well, population health management works: it improves health outcomes and can do so cost-effectively.
Frequently Asked Questions about Population Health Management
1. How is “population health management” different from “public health” or “community health”?
Population health management usually refers to efforts by healthcare organizations to improve health outcomes for a defined group of individuals, often their patients or members. It’s closely tied to healthcare delivery and uses medical data, care coordination, and clinical interventions.
Public health, on the other hand, is a broader field focused on protecting and improving health at a community or population level, often through policy, education, and prevention. Public health serves entire communities and is not limited to those in a health system. Community health is a related term that often focuses on health outcomes within a geographic community and can involve both public health and healthcare providers. In practice, these fields overlap; a hospital’s PHM program might collaborate with public health agencies on a vaccination drive, for example. But PHM is typically the term when healthcare providers take on accountability for outcomes for a specific population.
2. What kinds of organizations use Population Health Management?
Health systems and hospitals use PHM to manage patient populations, especially if they participate in value-based contracts or ACOs. Primary care groups and clinics use PHM to provide better preventative and chronic care. Insurance companies and managed care organizations employ PHM to improve member health and control costs, often coordinating with provider networks.
Accountable Care Organizations and other value-based enterprises rely heavily on PHM principles to achieve quality and savings targets. Even employers and government programs utilize PHM strategies. Essentially, any stakeholder who is responsible for the health outcomes of a group of people can benefit from PHM.
3. What are examples of data used in PHM that are not in a typical medical record?
PHM tries to be comprehensive, so it goes beyond the standard clinical data. Examples include:
- Claims data. Social determinants data like neighborhood socioeconomic status,
- Access to transportation, or
- Housing status.
Some PHM programs integrate data from social services or community programs. Pharmacy benefit data can show if a patient is refilling prescriptions on time. Lab results from outside labs, if not directly in the EHR. Increasingly, PHM may incorporate data from wearables or patient-reported outcomes surveys.
All these give a fuller picture of a person’s health and habits than the snapshot in an EMR. However, integrating these diverse data sources is a known challenge; it requires good data governance and consent management.
4. How does PHM relate to value-based care and reimbursement?
They are closely linked. Value-based care is all about reimbursing healthcare based on outcomes and quality rather than volume of services. PHM is essentially the toolset and approach to achieve success in VBC. For instance, under a value-based contract, a provider might get a bonus for keeping the population’s blood pressure under control or reducing hospital admissions. PHM provides the day-to-day processes to make those outcomes happen.
In models like ACOs, bundled payments, or patient-centered medical homes, providers take on risk for population health costs and quality. Without PHM, it would be very difficult to meet those benchmarks.
Conversely, if a healthcare organization is still mostly paid fee-for-service, the immediate financial incentive for PHM is less direct. Many organizations are adopting PHM ahead of payment changes, essentially preparing and improving care quality, knowing the industry is moving in that direction. And some value-based programs require certain PHM capabilities, e.g., CMS ACO programs require reporting of population quality measures that you really need PHM infrastructure to gather and improve.
5. What are common metrics tracked in Population Health Management?
PHM programs track a variety of clinical, utilization, and financial metrics. Common ones: Clinical quality measures such as HbA1c control in diabetics, blood pressure control in hypertensives, LDL control in cardiac patients, cancer screening rates, immunization rates, and medication adherence for chronic diseases. Utilization measures like ER visit rate per 1,000 patients, hospital admission rate, 30-day readmission rate, and avoidable hospitalizations.
Patient experience measures, such as patient satisfaction or engagement levels. If addressing SDOH, might track the number of patients with social needs addressed. Financial outcomes like total cost of care per patient, or savings achieved against a budget, are key in value-based scenarios. Example:
- An ACO might closely watch its per-member per-month cost trend,
- Hospitalization per 1000 trend, and
- Quality scores on a dozen chronic and preventive care indicators.
By seeing these metrics quarterly or monthly, they gauge if PHM interventions are working and where to adjust.
6. How do we measure the ROI of population health management?
Measuring return on investment for PHM can be multi-faceted. Direct ROI might be seen in reduced healthcare costs, for instance, fewer ER visits and admissions translating to lower spending for a payer or shared savings earned by a provider. If you’re an integrated system or capitated, you can compare cost trends before and after PHM implementation.
ROI can also be measured in improved quality scores and avoided penalties. Some ROI is long-term; preventing a chronic disease complication might not show dollar savings in year one, but over five years, the avoided hospitalizations or dialysis are huge.
Many organizations do cost-benefit analyses on specific programs: e.g., the cost of hiring 3 care managers vs the savings from prevented admissions among their caseload. If each care manager prevents X admissions, you can assign a dollar value. Another element is soft ROI:
- Improved patient satisfaction and
- Retention and improved provider satisfaction.
Those may not immediately translate to dollars, but they have organizational value. In summary, ROI can be quantified by blending utilization/cost data and quality improvements.
For example, one could report: “Our PHM program cost $500,000 this year, but it led to $1.2 million in savings from reduced hospital utilization, plus we earned a $300,000 quality bonus, net ROI of ~3:1, not even counting long-term benefits.” It’s important to track these, as leadership will want to see evidence that PHM is worth the investment.
7. What role do clinicians play in PHM? Do doctors have to do extra work?
Clinicians, especially primary care physicians, are central to PHM, but a well-designed program tries to distribute work across a team to avoid overburdening doctors. Physicians provide medical direction, setting care plans, making clinical decisions, and they often champion preventive care and chronic management in visits. They also might get alerts or reports on their patient panel’s gaps.
However, much of the outreach and coordination can be handled by support staff under protocol. For instance, a doctor might not personally call a patient who missed a visit, a care coordinator does that. Or a pharmacist might run a hypertension medication clinic to adjust doses between physician visits.
The idea is to optimize each team member’s role: let doctors handle complex decision-making and face-to-face care, while coordinating staff handle logistics and follow-up.
Initially, there may be a feeling of extra work if, say, doctors are asked to review performance dashboards or participate in care team meetings. But many organizations report that once workflows are adjusted, physicians appreciate PHM, which leads to healthier patients and provides help tackling issues they used to manage alone. The key is using a team-based care model: PHM is not the doctor doing everything; it’s the doctor plus an extended team enabled by data. Training and culture change are important so clinicians trust their team to carry out parts of care.
8. How long does it take to see results from a PHM program?
It depends on the outcomes targeted. Some improvements can be seen in the short term (6-12 months) , for example, if you implement a care gap closure program, you might see screening rates or immunization rates rise within a year. Reducing readmissions can also sometimes show results in a year or less with focused effort.
- For chronic disease metrics like blood pressure or diabetes control, significant population-level improvement might take 1-2 years as patients cycle through visits and titrations.
- Cost savings might lag a bit; you often invest upfront and see financial return after a year or two, once hospital utilization patterns change.
- Cultural shifts, like patient engagement and trust-building, can also take time.
- Many programs find that the first year is laying groundwork, cleaning data, stratifying, and outreaching to the highest-risk to stabilize them.
By the second year, trends like fewer ER visits or improved average risk scores become evident. Comprehensive evaluation is often done around the 3-5 year mark to capture things like reduced complication rates. It’s important to set expectations with leadership: PHM is not a “quick fix” but a structural change in care delivery.
That said, celebrating early wins within months of kickoff is important to keep momentum.
Patience and persistence are key; some initiatives might not show big numbers immediately, but steady gains compound. As one analogy goes: PHM is a marathon, not a sprint, but every mile in that marathon counts towards the finish.
Population Health Management Service Support by CapMinds
Turning PHM strategy into measurable outcomes takes more than a platform; it takes an engineering partner who can connect data, workflows, and governance end-to-end.
CapMinds helps providers, payers, ACOs, and community health programs operationalize Population Health Management with interoperability-first architecture, analytics enablement, and care coordination workflows aligned to value-based care.

CapMinds PHM services include:
- PHM platform implementation, configuration & optimization
- EHR + claims + lab + pharmacy data aggregation (FHIR/HL7/API integrations)
- Data normalization, patient identity matching & longitudinal records
- Risk stratification models, care gap analytics & executive dashboards
- Care management workflows (tasking, outreach, transitions of care)
- Patient engagement tools (portals, messaging, telehealth, RPM feeds)
- SDOH data capture, referral networks & equity reporting
- Security, HIPAA-aligned controls, governance & audit readiness
- Managed support, enhancements, performance tuning, and more
If your PHM roadmap is clear but execution is complex, CapMinds can build the integrated, scalable foundation to make it real.




