Healthcare Interoperability: HL7, FHIR & HIE Integration Explained

Healthcare delivery depends on information moving across a dense, heterogeneous mesh of systems: EHR/EMR platforms, laboratory information systems, radiology information systems, PACS archives, pharmacy and medication management, scheduling, billing and revenue cycle, registries, public health endpoints, remote monitoring platforms, patient portals, analytics warehouses, and identity services. In most organizations, these systems were not designed as a single coherent platform. They were acquired over the years, configured by different teams, upgraded on different cadences, and shaped by local workflows that differ not just across countries, but across hospitals in the same city.
Healthcare interoperability is the capability for these systems to exchange data, interpret it consistently, and use it meaningfully in downstream workflows, without manual re-entry, faxing, copy-paste, portal-only access, or ambiguous “human translation” at the point of care. Interoperability is not the same as “data exchange.” Many environments can exchange data and still fail interoperability because the receiving system cannot safely interpret, normalize, reconcile, and operationalize what arrives.
The most persistent gap in real-world interoperability is usable interoperability: whether the data is available at the right time, in the right context, linked to the right patient and encounter, aligned to shared semantics, and integrated into clinical and operational workflows. When interoperability fails, the consequences include redundant tests, delayed decision-making, unsafe medication reconciliation, inconsistent problem lists, administrative drag, denials from coding mismatches, incomplete quality reporting, and high integration maintenance costs.
Three concepts dominate modern interoperability engineering:
- Standards, which define “how to represent and move data.”
- HL7 v2 remains the workhorse for event-driven messages in many clinical environments.
- HL7 CDA/C-CDA is widely used for document-style exchange and transitions of care.
- FHIR is the modern API-first standard, built around resources, profiles, and web security.
2. HIE, which is both a process and a set of network/platform architectures to share data across organizational boundaries.
3. Operational discipline, which determines whether standards become reliable integrations: conformance contracts, terminology governance, identity management, event semantics, monitoring, incident response, and change control.

This guide is intentionally technical and global/neutral. It avoids policy-specific details tied to one region. It focuses on what engineering teams, architects, and integration leaders need to build, operate, and scale interoperability across multi-vendor ecosystems.
Interoperability in Healthcare Systems
Interoperability is often described as “systems exchanging and using data,” but that phrase hides why interoperability fails in practice. In a production healthcare environment, interoperability should be understood as a set of system guarantees your integration architecture must uphold across time, upgrades, and organizational change.
Data Integrity and Clinical Safety
Interoperability must preserve meaning. A medication list imported from an external source that misrepresents dose units is worse than no data. A lab result filed under the wrong patient due to an identity mismatch is a safety incident. “Correctness” here is not just schema compliance; it includes clinical interpretation constraints: units, reference ranges, coding semantics, timestamps, and provenance.
Timeliness and Workflow Alignment
Many workflows are time-bound. A clinician deciding whether to repeat a test needs results now, not “eventually.” An emergency workflow cannot wait for a minute-long federated query fan-out. “Timeliness” must be defined per use case, measured, and engineered.
Fitness-for-Purpose Data Scope and Completeness
Interoperability does not require that every system share everything. It requires that the shared subset is complete enough for the intended workflow, and that gaps are explicit. If allergies are partial, the consuming workflow must know they are partial. If only recent labs are available, the system must not imply longitudinal completeness.
Reliability, Resilience, and Operational Continuity
Healthcare integrations cannot be “best effort.” They must handle duplicates, retries, reprocessing, and partial outages without corrupting clinical state. A design that works when everything is up is insufficient. Resilience includes backpressure handling, error queues, replay controls, and idempotency strategies.
Traceability, Auditability, and Provenance
Clinical trust requires traceability: who authored this, which system generated it, when it was captured, how it was transformed, and whether it was reconciled. Provenance is often the difference between “data exists” and “data is used.”
Governance, Change Control, and Lifecycle Management
Interoperability is an operating model, not a one-time interface build. Standards evolve; vendors update; local workflows change; code sets update; security postures shift; certificates expire. An organization’s ability to manage these changes determines long-term interoperability cost and reliability more than initial implementation choices.
4 Interoperability Layers and Maturity Model
Interoperability is commonly broken into syntactic and semantic, but production-grade exchange requires two additional layers: organizational and workflow interoperability.
Syntactic interoperability
Syntactic interoperability means systems agree on structure and protocol: message segments and delimiters (HL7 v2), XML schemas (CDA), resource JSON structures (FHIR), and the transport patterns used to carry them. It answers: “Can the receiver parse what arrives?”
Syntactic interoperability is necessary, but often overestimated. Many systems parse data successfully and still cannot use it safely.
Semantic interoperability
Semantic interoperability means systems share meaning. This requires consistent use of coded terminologies, consistent modeling choices, and consistent constraints. It answers: “Does the receiver interpret the meaning the same way as the sender?”
Semantic interoperability depends on:
- code systems (e.g., lab test identification, diagnoses, medications)
- value sets (allowed codes for a field)
- units and measurement conventions
- profiles/constraints (especially in FHIR)
Semantic interoperability is where “standards without consistency” become visible. Two systems can both claim to support a standard and still differ in meaning.

Organizational interoperability
Organizational interoperability is about trust, authorization, consent, and accountability. It answers: “Should this data be shared, with whom, and under what conditions?”
Even with perfect technical exchange, organizations can block interoperability if authorization and governance are unclear. Conversely, weak governance can lead to over-sharing and security incidents.
Workflow interoperability
Workflow interoperability means external data is available in context, embedded in clinician and operational workflows, and supported by reconciliation and provenance. It answers: “Will users actually use the data without leaving their workflow?”
A common failure mode is “portal interoperability”: data is accessible but not integrated, so it is underused. This is a workflow problem with technical implications: latency, context passing, UI embedding patterns, reconciliation APIs, and event triggers.
HL7 Standards (HL7 v2, HL7 v3, FHIR)
HL7 has published a number of significant standards. Each has a distinct use case and focus:
Related: The Ultimate Guide to HL7 Standards: Everything Healthcare Providers Need to Know
HL7 v2 Messaging Architecture
HL7 v2 has remained central to healthcare integration because it solved a practical need early: event-driven messaging between operational systems in complex clinical settings. It is widely implemented, stable, and supported by countless legacy systems. But v2’s flexibility leads to variability, which creates an integration burden.
HL7 v2 Message Structure and Core Segments
HL7 v2 messages consist of segments separated by line breaks. Each segment begins with a three-character identifier such as MSH (Message Header), PID (Patient Identification), PV1 (Patient Visit), ORC (Common Order), OBR (Observation Request), OBX (Observation Result), and many others, depending on workflow.
Fields within segments are delimited by |. Components and subcomponents within fields use delimiters declared in MSH (commonly ^ and &). This delimiter-based approach is efficient and easy to transport, but requires careful parsing to handle optionality and repeating fields.
The MSH segment is foundational: it defines sending application, sending facility, receiving application, message type (e.g., ADT^A01), message control ID, and version. Many production issues trace back to assumptions about MSH fields, especially timestamps, control IDs, and encoding characters.
Event Semantics and Workflow-Driven Message Interpretation
HL7 v2 message types indicate categories, but not always precise semantics. For example, ADT events represent admissions, discharges, transfers, registrations, and updates. The specific meaning depends on local workflow configuration.
A message labeled “admission” might represent a registration event, a bed assignment, or an encounter status change, depending on the source system. Integration teams must model event semantics as a contract, not assume that HL7’s generic event label matches local operational meaning.
This becomes critical when downstream systems build state from events. If a downstream system uses ADT messages to infer patient location or encounter lifecycle, event semantics must be deterministic, or state drift occurs.
Acknowledgment Patterns (Transport vs Application Confirmation)
HL7 v2 workflows often rely on acknowledgments (ACK) to confirm message delivery and processing. Two concepts are commonly conflated:
- Transport-level receipt: the message arrived at the socket.
- Application-level acceptance: the receiving application parsed and accepted it.
In v2, the ACK message is the primary mechanism for application-level acknowledgment. But ACK behavior varies:
- Some systems ACK upon receipt (before business validation).
- Some ACK only after parsing and validation.
- Some send negative acknowledgments for specific errors, but others silently drop or route to error queues.
A robust architecture separates:
- receiving durability (store the message safely upon receipt)
- processing and validation (can fail and be retried)
- acknowledgment semantics (should reflect the right layer)
If the sender retries based on ACK absence, and the receiver ACKs too early, you risk acknowledging messages that later fail processing. If the receiver ACKs too late, you risk duplicates due to timeout retries.
Transport Mechanisms and Operational Constraints (e.g., MLLP)
MLLP over TCP is common for v2 because it is simple. But it has implications:
- Persistent connections must be monitored and restarted
- Network interruptions create partial message risk
- TLS is not inherent; security depends on the network and wrappers
- Throughput scaling is often connection-bound
At scale, organizations often use interface engines to terminate MLLP connections, persist messages, and manage downstream routing. This is a practical pattern to isolate legacy transport constraints from modern processing architectures.
Idempotency, Duplicate Handling, and Replay Control
HL7 v2 systems commonly send duplicates due to retries, network failures, or operational replays. Receiving systems must assume duplicates are normal, not exceptional.
Idempotency strategies typically rely on:
- message control ID (MSH-10) as a transaction identifier
- event timestamp and patient/encounter keys
- receiver-side deduplication windows
- strict rules about when reprocessing is safe
However, message control IDs are not universally stable across replays. Some systems regenerate control IDs. Some replay historical messages with new IDs. Therefore, deduplication often requires composite keys and state-aware logic.
Sequencing, State Management, and Encounter Lifecycle Modeling
Many v2 workflows are stateful. ADT messages can be interpreted as transitions in an encounter state machine: created, admitted, transferred, discharged, corrected, merged, etc. If messages arrive out of order, the state machine can become inconsistent.
A robust design:
- defines a formal state model for encounters
- defines which events are authoritative
- defines correction mechanisms (e.g., A08 updates)
- handles late-arriving events (reconciliation rules)
- implements reprocessing with state rebuild capability
Without explicit state modeling, teams end up with fragile ad hoc rules that break during upgrades.
Validation Strategy: Structural vs Business Rule Enforcement
HL7 v2 validation must be layered:
- structural validation: segment presence, field delimiters, data types
- business rule validation: required fields for a workflow, code system constraints, reference integrity
- semantic validation: local-to-standard mappings, unit checks, allowable value sets
Structural validity does not guarantee business correctness. For example, an OBX segment can be structurally valid, but it may use a local code that downstream systems cannot interpret.
Why HL7 v2 Remains Foundational in Clinical Integrations
HL7 v2 persists because it is embedded, widely supported, and well-suited to event messaging in controlled networks. It is also highly adaptable through local conventions, which makes it usable everywhere. That same adaptability is the reason it creates interoperability debt: every interface becomes its own contract.
HL7 v3 and Clinical Document Exchange (CDA/C-CDA)
HL7 v3 attempted to formalize healthcare data exchange with a model-driven approach. While v3 messaging did not replace v2 broadly, the v3 era produced CDA (Clinical Document Architecture), which remains central for document exchange.
CDA Fundamentals: Document Structure and Metadata
CDA is an XML-based standard for clinical documents. A CDA document includes:
- metadata about author, organization, encounter context
- a narrative portion readable by humans
- structured entries for coded data sections
CDA’s design makes it resilient as a communication artifact: even if structured parsing is imperfect, the narrative is readable. This is a practical property in clinical environments where completeness and interpretability matter.
Template-Based CDA and Constrained Implementation Models
CDA is flexible, so template frameworks emerged to constrain it for specific document types. “Consolidated CDA” (C-CDA) is a known approach where specific templates define how to represent common clinical summaries. The intention is to reduce variability and increase computational efficiency.
In reality, template conformance varies. Two systems can both claim to support a CDA document type and still diverge in how they populate coded entries.
Operational Reality: Document-Centric Exchange vs Computable Data
CDA frequently becomes “view-only interoperability.” Systems store documents as attachments or external references, and clinicians must open them separately. Even if the document contains coded entries, the receiving system may not reconcile them into local structured lists.
This happens for reasons that are more operational than conceptual:
- Parsing and reconciliation require significant engineering effort
- Different sections and templates must be handled
- Data reconciliation requires workflow governance and user interaction
- Provenance and trust decisions must be built into UI and clinical workflows
Appropriate Use Cases for CDA-Based Interoperability
CDA remains appropriate when:
- A complete narrative snapshot is required
- The receiving side needs a self-contained artifact
- Legal/completeness requirements favor document packaging
- Systems cannot support fine-grained APIs reliably
CDA is less appropriate when the workflow requires only specific data elements, or when low latency and structured reconciliation are key.
CDA-to-FHIR Harmonization and Transformation Approaches
FHIR can represent document exchange via Composition and Bundle patterns. Many architectures treat CDA as an inbound/outbound artifact while maintaining internal canonical structured representations. A common approach is to ingest CDA, parse key entries, map them into canonical structures, and expose them through FHIR or internal APIs.
Related: Designing a Central Interoperability Hub: HL7 v2, FHIR, CCD, and Direct Messaging
FHIR API-Based Interoperability
FHIR is often described as “HL7 for modern APIs,” but the deeper value is its combination of:
- a resource-based data model
- standardized REST operations and search
- extensibility and profiling
- conformance artifacts and validation tooling
- security patterns aligned with mainstream API ecosystems
FHIR is not just a format. It is a platform for building interoperable API ecosystems. Its success depends on discipline: profiles, terminology binding, conformance testing, and operational governance.
FHIR Resource Model and Clinical Data Modularity
FHIR resources are the building blocks. Each resource defines a set of fields, data types, and references to other resources. The modular approach avoids monolithic documents by enabling the retrieval and updates of specific concepts.
Resource references enable assembly of clinical context across resources: Observations reference Patients, Encounters, and Practitioners. Medication-related resources reference Patients and ordering providers. This graph-like structure matches many real-world use cases.
RESTful Interactions: Read, Search, Create, Update, Patch
FHIR defines standard interaction patterns using HTTP:
- read: retrieve a resource by ID
- search: query resources using parameters
- create: create new resources
- update/patch: modify existing resources
FHIR search is particularly important because it standardizes a large category of “integration needs” that otherwise become bespoke API endpoints. A system can query for specific Observations, Conditions, or Encounters using shared search semantics.
However, search in production is only as good as the server implementation. Performance constraints, indexing strategies, and parameter support vary widely. This is where conformance artifacts matter.
Search Semantics: Filtering, Sorting, Pagination, and Includes
FHIR search supports:
- filtering by parameters (patient, code, date, status, etc.)
- pagination (server returns pages of results)
- sorting (order results by a field)
- includes (fetch referenced resources alongside results)
In large environments, search design becomes an architectural issue. If a use case requires retrieving large sets of data frequently, naive search can overload servers. Solutions include:
- caching and prefetching
- bulk data export for analytics workflows
- event-driven updates rather than repeated searches
- limiting search scopes via compartments or access tokens
Bundles and Packaging Patterns (Search, Transaction, Document)
FHIR bundles package multiple resources in one response. Bundles are used for:
- search result sets
- transactions (multiple creates/updates in one request)
- documents (Composition + Bundle)
- messaging-like workflows (less common but possible)
Bundles are essential when you need a multi-resource context without many round-trip requests.
Conformance and Capability Modeling (Capabilities, Profiles, IGs)
FHIR introduces explicit conformance artifacts:
- CapabilityStatement: describes what a server supports (resources, interactions, search params, profiles)
- StructureDefinition: defines a profile (constraints on resources)
- ValueSet and CodeSystem: define terminology constraints
- Implementation Guides: publish a coherent set of profiles and rules for a domain
In practice, FHIR interoperability is profile-driven. Base resources are flexible. Profiles define what “this field is required,” “these codes are allowed,” and “this resource must look like this in this ecosystem.”

Extensions and Profiling Strategy: Flexibility with Governance
FHIR allows extensions to add fields not present in base resources. Extensions are identified by URIs and can be defined in a profile. This enables local requirements without breaking the base standard.
But extensions must be governed:
- Uncontrolled extensions produce fragmentation
- Consumers cannot interpret unknown extensions without documentation
- Excessive extension use can replicate the “local dialect” problem seen in HL7 v2
A mature architecture uses extensions sparingly and prefers standard fields where possible.
Versioning Strategy and Backward Compatibility Management
FHIR has multiple versions in the ecosystem. Even if one version dominates, version drift is inevitable over time. Production systems need explicit strategies:
- API versioning at gateways (e.g., /fhir/r4/…)
- profile versioning (and backward compatibility guarantees)
- compatibility testing during upgrades
- consumer migration plans
A common failure mode is “FHIR endpoint exists,” but consumers break when the provider upgrades and profile behavior changes without versioning discipline.
Implementation Risks
FHIR reduces integration friction, but it does not automatically fix:
- poor data quality
- missing structured capture
- inconsistent coding discipline
- identity issues
- workflow embedding challenges
FHIR is best seen as a modern interoperability substrate. Success depends on the ecosystem constraints imposed through implementation guides, governance, and conformance tooling.
Related: The Complete Guide to FHIR in Healthcare: Architecture, Use Cases, and Implementation
Selecting HL7 v2, CDA, or FHIR for Specific Integration Requirements
Many organizations waste effort trying to replace one standard with another universally. In practice, interoperability is mixed-mode. The correct choice depends on workflow needs, system capabilities, and operational constraints.
Decision Criteria: Latency, Granularity, Security, and Workflow Fit
Key decision factors include:
- latency requirements (seconds vs minutes vs hours)
- granularity (single lab result vs whole record summary)
- sender capabilities (legacy departmental system vs modern API platform)
- receiver workflow (automated reconciliation vs narrative review)
- security and authorization model requirements
- ecosystem expectations (apps, analytics, cross-org exchange)
Comparative Evaluation: Practical Trade-offs Across Standards
| Dimension | HL7 v2 | CDA (C-CDA) | FHIR |
| Primary shape | Event messages | Clinical document | Resource API |
| Typical transport | MLLP/TCP, files | secure transport, portal, messaging | HTTPS/REST |
| Best for | event feeds, results streams | transitions of care snapshots | fine-grained access, app ecosystems |
| Semantic consistency | variable; local dialects | variable; template discipline needed | depends on profiles; improves with IGs |
| Workflow integration | strong internally | often view-only | strong if embedded via apps/APIs |
| Security model | external (network-based) | external + document controls | OAuth/OIDC patterns are possible |
| Operational maturity | high in legacy ecosystems | high for document workflows | rapidly maturing |
Recommended Patterns for Mixed-Mode Interoperability (Coexistence)
HL7 v2 is most appropriate for event-driven operational integration, especially inside organizations or with partners using legacy connectivity. CDA is most appropriate for narrative-rich summaries and transitions of care snapshots. FHIR is most appropriate for API-first interoperability: apps, patient access, analytics services, and flexible retrieval where web security and granular queries are required.
Mixed-mode architectures typically ingest HL7 v2 and CDA, normalize them into a canonical model, and expose a consistent FHIR API surface for consumption.
Health Information Exchange Architecture Models
A Health Information Exchange is both a process and a set of platform/network architectures that enable exchange across organizations that do not share a single EHR. HIEs solve problems that pure point-to-point interfaces cannot solve reliably:
- identity matching across organizations
- endpoint discovery and trust frameworks
- consent and policy enforcement
- normalization across heterogeneous sources
- scalable query and notification workflows
Centralized HIE (Repository-Oriented Architectures)
In a centralized model, the HIE maintains a central repository where participants contribute data. Participants push updates via feeds or documents; the HIE stores, indexes, and serves data to authorized requesters.
Centralized HIEs can deliver lower-latency queries because data is pre-aggregated and indexed. They can also apply normalization centrally, improving semantic consistency.
However, centralized HIEs carry a higher operational burden:
- They are major PHI repositories with high security requirements
- Governance complexity increases (data stewardship, retention, access policies)
- Contribution workflows require consistency and continuous onboarding effort
Federated HIE (Source-Resident Data Architectures)
In a federated model, data remains at the source organizations. The HIE provides:
- A record locator service (where data exists)
- Identity services (matching patients)
- Orchestration for queries and retrieval
Federated HIEs reduce central storage and can be easier to govern in terms of data custody, but they introduce:
- Latency risk: queries must fan out to multiple sources
- Availability dependency: if a source is down, data is unavailable
- Merging complexity: combining heterogeneous responses in real time
- Identity challenges: matching at query time is harder than during ingestion
Federated models often struggle when workflows require near-instant results at the point of care.
Hybrid HIE (Caching + Federated Retrieval Architectures)
Hybrid models blend centralized caching/summaries with federated retrieval for deeper content. This can take multiple forms:
- store summaries centrally; retrieve full details from sources on demand,
- cache frequently accessed data for high-value workflows,
- operate as “network-of-networks,” with multiple HIE nodes interconnected
Hybrid models are common in large-scale ecosystems because they balance performance, governance, and operational feasibility.
HIE Exchange Workflows and Standards Utilization
HIEs typically support multiple exchange workflows simultaneously because participants have different technical capabilities and the ecosystem evolves.
Event Feeds and Push-Based Data Contribution
Many HIEs rely on event feeds to populate repositories or enable alerts. Common feed patterns include patient movement events (admissions, discharges, transfers), results feeds, and other operational signals.
Event-driven push enables:
- alerts and notifications to care teams
- near-real-time longitudinal updates in centralized models
- trigger-based workflows (care coordination, follow-up, population health)
The engineering challenge is that event feeds vary in quality and semantics. To make them clinically useful, the HIE must manage:
- deduplication
- event ordering issues
- identity linkage accuracy
- code and unit normalization
- provenance metadata for trust
Clinical Document Exchange Workflows
Document exchange remains central for transitions of care. Document workflows are valuable because they provide a complete snapshot that can be read even when structured ingestion is limited.
However, document workflows often struggle with:
- inconsistent template population
- limited structured reconciliation
- slow retrieval in federated settings
- user workflow friction (opening documents outside the main EHR flow)
Related: Optimizing Mirth Connect Channels for High-Volume CCD/C-CDA Document Workflows
Query-and-Retrieve Models (On-Demand Data Access)
Query/retrieve workflows enable a provider to request data for a patient on demand. Architecture determines how it behaves:
- centralized: query repository, return results quickly
- federated: locate records, query sources, merge responses
Query/retrieve becomes usable in time-bound workflows only when:
- Identity matching is fast and accurate
- The record location is reliable
- Caching/prefetching reduces latency
- The receiving EHR can integrate responses into the workflow
API-Led HIE Models and FHIR Enablement Patterns
Modern HIEs increasingly expose APIs as a unified interface, even when they ingest multiple standards. The common architectural approach is:
- Ingest HL7 v2 and CDA from participants
- normalize into a canonical model
- expose data via FHIR resources, constrained by profiles
This creates a consistent developer surface, supports app ecosystems, and enables modern authorization patterns. It also shifts the HIE’s role toward being a normalization and governance layer, not just a transport network.
Canonical Data Architecture and Integration Middleware Patterns
Point-to-point interfaces scale poorly. Each new system introduces multiple new mappings, monitoring points, and change risks. A canonical model reduces integration complexity by establishing a standard internal representation.
Scaling Constraints of Point-to-Point Integration Topologies
In point-to-point architectures, each system must map to every other system. As the number of systems grows, the number of interfaces grows roughly quadratically. Maintenance effort grows even faster because each interface is affected by upgrades, code changes, and workflow changes in either endpoint.
Point-to-point integration can be reasonable in small ecosystems, but it becomes brittle and expensive at scale.
Canonical Data Models and Normalization Layers
A canonical model architecture uses a hub-and-spoke approach:
- each producer maps into a canonical representation
- each consumer maps from the canonical representation
This reduces the number of mappings and centralizes governance:
- Terminology normalization can be performed centrally
- Identity cross-references can be maintained centrally
- Validation rules can be standardized
- Monitoring can be consolidated
A canonical model can be implemented as:
- A canonical database schema
- Canonical event stream
- A canonical FHIR server (with profiles) used as the internal model
- A hybrid (event stream + materialized stores)
End-to-End Transformation Pipelines: Ingestion, Processing, Distribution
A mature pipeline typically includes:
- Ingestion (receive and persist raw messages/documents)
- Parsing and structure validation
- Identity resolution (link to enterprise patient IDs)
- Terminology normalization and unit checks
- Transformation into canonical structures
- Enrichment (provenance, encounter linking, source metadata)
- Routing to consumers (internal systems, HIE outputs, analytics)
- Mirth Connect audit logging and monitoring across each integration stage.

Crucially, the pipeline must be replayable. When mappings change, the system should be able to reprocess historical messages safely (subject to governance policies).
Identity Resolution and Patient/Provider Linking
Identity is the most safety-critical interoperability problem. Perfect schema compliance is useless if data is attached to the wrong person.

Identity Challenges in Multi-System and Cross-Organization Exchange
Healthcare identity is difficult because:
- There is no universal patient identifier in many contexts
- Demographic data is inconsistent and changes over time
- Multiple identifiers exist across systems (MRNs, local IDs, payer IDs)
- Data entry errors are common
- Duplicates and overlays occur
Even within one organization, identity mismatches occur when departmental systems maintain separate identifiers or when integration cross-references drift.
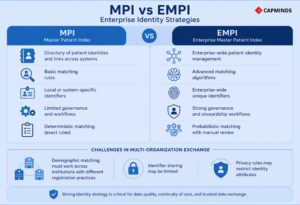
MPI vs EMPI: Enterprise Identity Strategies
A Master Patient Index maintains a directory of patient identities and links across systems. An Enterprise Master Patient Index (EMPI) typically implies:
- more robust matching algorithms
- enterprise-wide unique identifiers
- governance and stewardship workflows
- probabilistic matching with manual review
In a multi-organization exchange, identity becomes harder because:
- Demographic matching must work across institutions with different registration practices
- Identifier sharing may be limited
- Privacy rules may restrict identity attributes
Matching Approaches: Deterministic and Probabilistic Methods
Deterministic matching uses exact matches on identifiers. It is highly accurate when identifiers are reliable and shared.
Probabilistic matching uses weighted comparisons across demographics (name, date of birth, address, phone, etc.). It can improve match rates but introduces risk:
- False positives (incorrect matches) are safety incidents
- False negatives (missed matches) reduce interoperability value
A mature identity strategy includes thresholds, manual review queues, and auditing for merges and splits.
Identifier Cross-Reference Management and Data Linking Controls
Integration engines and canonical systems often maintain cross-reference tables:
- system A patient ID ↔ enterprise patient ID
- system B patient ID ↔ enterprise patient ID
- provider IDs across systems
- encounter IDs across systems
Cross-reference integrity must be monitored. When cross-references drift or break, downstream systems can silently attach data incorrectly.
Identity Representation in FHIR
FHIR resources support multiple identifiers with system URIs, which helps carry multiple identity contexts in a structured way. However, this still requires governance: which identifier is authoritative for which workflow, and how duplicates are handled.
Semantic Interoperability and Terminology Services
Semantic interoperability is the difference between “data received” and “data usable.”
Sources of Semantic Variability Across Systems
Semantics fail when:
- Local codes are used instead of standardized codes
- Units differ or are missing
- The same code is used inconsistently across contexts
- Fields are populated differently across systems
- Profiles and constraints are not enforced
Even with FHIR, semantics fail if resource fields contain locally meaningful codes that consumers cannot interpret.
Terminology Service Capabilities (Validation, Mapping, Versioning)
A terminology service supports:
- Management of code systems and versions
- Validation of codes against value sets
- Mapping between local codes and standard codes
- Expansion of value sets for UI selection or validation
- Unit normalization support
- Audit trails for mapping changes
Terminology management is not a “nice-to-have.” It is required for sustainable interoperability in heterogeneous ecosystems.
Normalization Placement: Source vs Middleware vs Consumer
Normalization can be performed at multiple points:
- At source systems (ideal but rarely consistent)
- In integration middleware (common and practical)
- In HIE processing pipelines
- At the consumer (least desirable because it duplicates work)
A scalable approach centralizes normalization as close to ingestion as feasible, so all consumers benefit from consistent semantic processing.
Value Sets, Profiles, and Enforceable Semantic Constraints
FHIR profiles can specify required value sets for coded fields. This is a powerful way to enforce semantic consistency. But enforcement must be operationalized:
- Validators must be in the pipeline
- Failing data must be handled (reject, quarantine, or map)
- Governance must define acceptable exceptions
Without enforcement, value set definitions become documentation rather than a contract.
Event-Driven Interoperability and Real-Time Integration
Batch exchange is often incompatible with modern workflows. Event-driven interoperability reduces latency and improves consistency across systems.
Streaming HL7 v2 and Real-Time Message Processing
HL7 v2 can function as a near-real-time stream when:
- Events are emitted promptly by source systems
- Messages are processed continuously by the middleware
- downstream systems can ingest events reliably
- Backpressure and retry mechanisms exist
In many environments, v2 feeds are the practical starting point for event-driven interoperability because they already exist.
Event Bus and Pub/Sub Architecture for Clinical Events
Introducing an event broker or event bus can improve scalability:
- One event can be consumed by many downstream systems
- Replay and durability can be centralized
- Producers and consumers are decoupled
- New consumers can be added without changing producers
This is particularly useful when the same event must update clinical systems, billing, analytics, and notifications simultaneously.
FHIR Subscriptions and Notification-Based Integration
FHIR defines subscription mechanisms for notifying clients when resources change. In practice, adoption and support vary, but the underlying pattern is important: move from polling to push notifications.
When implemented well, subscription patterns:
- Reduce load from repeated searches
- improve timeliness for high-value workflows
- enable proactive workflow embedding (data arrives before the user asks)
Subscription patterns must still address:
- authorization and consent constraints
- rate control and event storms
- reconciliation with eventual consistency and retries
Trigger-Driven Prefetching and Workflow-Aware Data Delivery
Many workflows become usable only when data retrieval is proactive.
For example, when a patient is registered or admitted, systems can prefetch relevant external data so it is available by the time the clinician opens the chart. This requires:
- clear trigger events (registration, admission, referral creation)
- identity resolution early in the workflow
- caching and expiration rules
- provenance labeling and reconciliation logic
Security, Privacy, and Trust for Interoperability
Interoperability expands the attack surface. Multiple endpoints, multiple transports, and distributed trust require deliberate security architecture.
Transport Security and Network Protections
Legacy transports like MLLP require additional measures:
- VPN tunnels or private network routing
- TLS proxies/wrappers
- strict network segmentation
- firewall rule management
Modern API-based exchange typically uses TLS/HTTPS, but TLS is only the baseline.
Authentication and Authorization Models (Token, Role, Context)
API interoperability requires strong authentication and authorization. OAuth2 and OpenID Connect patterns support:
- token-based access
- scoped authorization (least privilege)
- user-context access (who is making the request)
- delegated consent (where applicable)
- revocation and auditability
Authorization must include policy enforcement beyond the technical scope:
- patient context restrictions
- role-based access
- purpose-of-use constraints (where required)
- break-glass workflows and auditing
Audit Logging, Non-Repudiation, and Access Monitoring
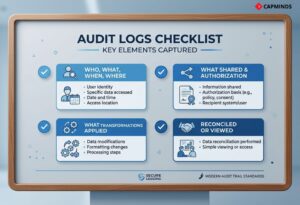
Audit logs should capture:
- Who accessed what data, when, and from where
- What was shared and under what authorization context
- What transformations were applied
- Whether the data was reconciled or simply viewed
Auditing is not just for compliance. It is an operational requirement for debugging and trust.
Provenance, Source Attribution, and Data Lineage
Provenance enables clinical trust. Key provenance concepts include:
- source system identity
- author and organization context
- capture time vs transmission time
- transformation history (mappings, normalization steps)
- confidence indicators (e.g., whether identity match was deterministic or probabilistic)
FHIR includes provenance concepts as resources, but provenance can be implemented in other forms as well. The key is that provenance must be accessible to workflows, not hidden in logs.
Testing and observability: validation gates, monitoring, SLOs, replay
Interoperability systems often fail quietly. Without observability, organizations discover failures only when clinicians complain or quality reports break.
Validation Gates: Schema, Business Rules, and Semantic Checks
Validation must be layered:
- structural validation (schema/message format)
- business rule validation (required fields, workflow constraints)
- semantic validation (terminology, units, allowed value sets)
- referential integrity checks (patient/encounter existence, identifier cross-references)
A robust pipeline treats validation failures as first-class events:
- quarantine data to error queues
- provide triage tooling
- avoid silent drops
- allow safe reprocessing after correction
Monitoring and Telemetry: Throughput, Errors, and Latency
Mature monitoring includes:
- throughput by interface and message type
- processing latency percentiles
- error rates and error category breakdowns
- queue depth and backpressure indicators
- endpoint availability and connection health
- certificate expirations and auth failures
Monitoring should support alerting on anomalies:
- Sudden drops in volume (source outage)
- Spikes in errors (schema drift)
- Increased latency (downstream slowdowns)
- Replay storms (operational issues)
Service Objectives (SLOs) for Integration Reliability
Interoperability should have service objectives, such as:
- message delivery latency targets for critical feeds
- maximum acceptable error rate
- recovery time objectives for interface outages
- The maximum time data can remain in quarantine before triage
SLOs drive staffing models, tooling investments, and prioritization. Without SLOs, interoperability becomes reactive.
Replay, Backfill, and Safe Reprocessing Mechanisms
Replay is essential. When mappings change or when an outage occurs, teams must be able to reprocess data safely. Replay architecture requires:
- durable storage of raw inbound payloads
- versioned transformation logic
- idempotent processing strategies
- careful policies for historical corrections
Without replay, teams resort to manual patching and ad hoc fixes that increase risk.
Interoperability Challenges in Production
Even with modern standards and careful implementation, challenges persist in healthcare interoperability. Some of the key ongoing challenges include:
Semantic Variability
Different systems might label and structure data differently, which can lead to misinterpretation.
- For instance, one EHR might use a custom code for a lab test that another doesn’t recognize, or might omit a data element that others include.
- This lack of semantic alignment means the receiving system might get data but not “understand” it fully.
- Continued efforts in standardizing code sets (LOINC, SNOMED, ICD) and using FHIR profiles/Implementation Guides are needed to close this gap.
In the U.S., the US Core Data for Interoperability defines a set of data classes to exchange, but a recent survey found only about 40% of HIE organizations routinely send data fully aligned with USCDI, and only ~33% receive such standardized data.
This indicates many exchanges still have content that isn’t normalized to national specs, a challenge that needs to be addressed through better data governance and tooling.
Data Quality and Completeness
Sharing data is only helpful if the data is accurate and complete. Studies show that 15–30% of key clinical data elements may be missing in many EHRs. If one hospital doesn’t capture a patient’s allergies, that allergy won’t magically appear via interoperability. Likewise, if data is entered in free-text in one system, it might not map cleanly to a structured form in another.
As healthcare moves toward data-driven decision support and population health, data completeness is becoming as critical as connectivity. This challenge goes beyond interoperability into clinical data entry practices and EHR design, but it affects the value of exchanged data. One missing piece of information can cause clinicians to mistrust the whole external dataset.
Latency and Performance
Users expect instantaneous information. If an HIE query takes 30 seconds or a minute, that’s often too slow in a clinical workflow. Ensuring that queries (especially federated ones) are optimized is tricky.
- Caching strategies,
- Index optimization, and
- Potentially employing event-driven pushes is are approach to mitigate this.
The future may involve more FHIR subscriptions and event notifications to pre-fetch data before a user even asks (for example, notify a primary doctor’s system as soon as their patient is seen in an ER, so that by the time the doctor looks, the data is already there).
Overcoming legacy system slowness is part of this – some older systems just can’t handle high query volumes, which is why a middle-tier or data repository is often introduced.
Integration of “Cost” and Sustainability
Building and maintaining interfaces is expensive. Every custom mapping, every new connection has a cost. One hidden issue in healthcare is that many integrations are one-off projects funded by initial implementation budgets, but there’s often insufficient funding for ongoing maintenance and upgrades.
This leads to technical debt and interfaces running on outdated standards or technology. Efforts like standardized FHIR APIs aim to reduce cost by making integrations more plug-and-play, but in the interim, organizations have to plan financially for integration as an ongoing service (include it in IT budgets, get support from leadership by demonstrating the value).
On a larger scale, HIE networks have struggled with sustainability – many rely on grants or subscription models that can be hard to maintain. The good news is that as interoperability moves from a “nice-to-have” to a regulated must-have (e.g., through national mandates), funding and prioritization are improving.
Privacy, Consent, and Trust
Technically, ensuring privacy (as discussed) is a challenge but manageable with encryption and access controls. The harder part is inter-organizational trust and patient consent. Different regions have different laws about what data can be shared and under what conditions.
- For example, behavioral health or substance abuse records may have extra restrictions. Implementing those rules in an automated way is complex.
- Some HIE software now includes consent management modules to record patient choices (opt-out, or selective sharing choices).
- The future likely involves more patient-mediated exchange – where patients control apps that aggregate their data via FHIR and then share it as they wish.
- That flips some of the paradigm, but it will coexist with provider-mediated exchange. Interoperability efforts will need to continue focusing on robust consent frameworks.

Information Blocking and Vendor Behavior
Non-technical but impactful, some system vendors or providers have historically been reluctant to share data freely due to competitive or business reasons.
Regulations in the US now prohibit unjustified blocking, but monitoring and enforcement are still evolving. Technically, you might find an EHR that has a FHIR API but limits its throughput or requires high fees for third-party connections.
Overcoming these hurdles requires not just tech but policy and market pressure. As APIs become the norm, we expect such resistance to decrease, but integration teams should be prepared to handle proprietary quirks or negotiate access.
Future Outlook for Health Interoperability
Looking ahead, the future of healthcare interoperability seems to be converging on a few trends:
Nationwide/Global Networks
There’s movement towards linking local exchanges into larger networks (e.g., the envisioned U.S. Network of Networks via TEFCA). Technically, this means more standardized protocols at a national scale (potentially FHIR-based for certain queries, and a national directory of endpoints). It also means scaling issues need to be solved (lookups across millions of patients and thousands of organizations).
FHIR Ecosystem Maturity
FHIR is continuously evolving (FHIR R4 is widely deployed; FHIR R5 was recently published with incremental updates). Tooling around FHIR – like FHIR-based analytics, clinical reasoning (decision support) – will grow.
Also, bulk data transfer via FHIR (for research or population health) will become more commonplace, as already seen with CMS requiring payers to use FHIR to share claims data in bulk. FHIR will not completely replace HL7 v2 in the near term, but in new integration domains (like patient-facing apps or quality reporting), it has basically taken over.
Event-Driven Healthcare (Subscriptions, Webhooks)
We anticipate broader use of event notifications. HL7 is working on standards like HL7 FHIR Subscription/Notify, and IHE is working on profiles for push notifications.
Imagine a future where, instead of polling an HIE for new info, a provider’s system can subscribe to a patient’s data and automatically get a FHIR notification resource whenever something changes (e.g., a new lab result is available or a care transition occurred). This would greatly reduce latency and lighten the cognitive burden on clinicians to “go look for info.”
Artificial Intelligence and Data Use
With more data flowing, there’s a huge interest in applying AI/ML to healthcare data. Interoperability will play a role in feeding those algorithms comprehensive data.
- Conversely, AI might assist in interoperability – for example, using natural language processing to map unstructured or mismatched data to standard terminologies.
- AI might also help with patient matching and detecting data anomalies across systems.
Patient-Centric Data Exchange
Personal health records and patient-controlled data exchange will likely increase. This doesn’t replace provider HIE, but complements it. It means integration strategies should include enabling patients to connect and retrieve their data.
This is already mandated in some places – e.g., U.S. certified EHRs must allow patients API access. By empowering patients, some of the interoperability burden is handled by the patient’s initiative (they carry their data in an app). But it introduces new challenges: ensuring those apps are secure and that patients understand the data.
Key Takeaways for Healthcare IT Leaders
Healthcare interoperability is defined by usable integration, not by transport capability. HL7 v2 remains central for event messaging and operational feeds, but it requires strict interface contracts, validation, and mapping discipline to avoid “local dialect” chaos. CDA remains valuable for narrative-rich clinical summaries, but it often becomes view-only unless systems invest in parsing, normalization, and reconciliation workflows. FHIR modernizes interoperability through resource APIs, profiles, and conformance tooling, but it only delivers real interoperability when ecosystems adopt consistent implementation guides, enforce terminology bindings, and operate disciplined versioning and testing.
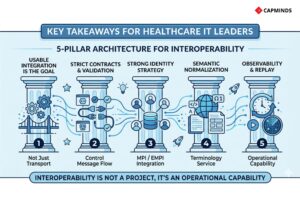
At scale, the most resilient approach is architectural and operational: a canonical model with transformation pipelines, a strong identity strategy (MPI/EMPI and cross-reference integrity), a terminology service for semantic normalization, event-driven patterns for timeliness, and robust observability with replay capability. Interoperability is not a project; it is an operational capability.
Frequently Asked Questions (FAQ)
1) Is interoperability primarily a standards problem or an implementation problem?
It is primarily an implementation and governance problem. Standards define structure and patterns, but usability depends on semantics, identity, workflow embedding, monitoring, and change control.
2) Why do HL7 v2 integrations require so much customization?
HL7 v2 is flexible and optional, leading to local variations, custom segments, and inconsistent field usage. Each interface becomes a contract that must be mapped, validated, and maintained.
3) If we adopt FHIR, will interoperability become plug-and-play?
Not automatically. FHIR reduces integration friction and provides conformance mechanisms, but real interoperability depends on profiles, terminology discipline, identity resolution, and testing.
4) Why do document exchanges often fail to produce computable data?
Because parsing and reconciling document sections into structured lists requires engineering effort and workflow governance. Many systems treat documents as attachments because it is a simpler operationally.
5) What is the biggest safety risk in interoperability?
Incorrect identity matching (data attached to the wrong patient) and semantic misinterpretation (wrong units or codes) are the most serious safety risks.
6) Should we aim to replace HL7 v2 with FHIR everywhere?
Most ecosystems will be mixed-mode for years. A practical strategy is to normalize v2 and CDA into a canonical model and expose consistent FHIR APIs for modern consumption, while keeping v2 where it remains operationally appropriate.
CapMinds Healthcare Interoperability Service Advantage
Interoperability only delivers value when HL7 v2 feeds, FHIR APIs, and HIE workflows are engineered as an operating capability, not a one-time interface project.
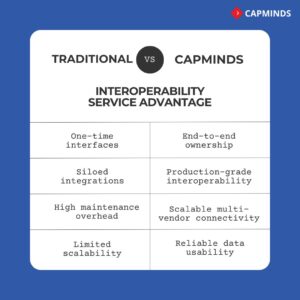
CapMinds provides end-to-end health interoperability services that reduce integration debt, improve data usability, and keep exchange reliable across vendor upgrades, workflow changes, and scaling demands.
- HL7 v2 Interface Development & Modernization
- FHIR API Engineering & Profiling
- HIE Integration & Network Connectivity
- Integration Middleware & Canonical Data Architecture
- Identity & EMPI/MPI Enablement
- Terminology & Semantic Normalization Services
- Security, Auditability & Observability
- Managed Interoperability Operations and More
If you need scalable, production-grade interoperability across multi-vendor ecosystems, CapMinds can own the delivery end-to-end.




